[12:09, 12/5/2022] Gustavo Zubieta: Dear Dr. Meera: [12:10, 12/5/2022] Gustavo Zubieta: Wonderful article! Very detailed and extensive. Congratulations, well done!!! Thank you for citing me!! All the best!! [12:12, 12/5/2022] +91 86100 66441: 🙏💐it was a pleasure to have met the scientific community through the conference. Your thoughts and work mean a lot to ayurveda. It will establish ayurveda’s scientificity in the long run.. A few centuries from now.. [12:13, 12/5/2022] +91 86100 66441: You are much ahead.. Our world is much behind Dr Gustavo [12:19, 12/5/2022] Gustavo Zubieta: I am truly impressed on how you have interpreted our work. Splendid because you understand the concepts!!! Ayurveda has great wisdom instilled, and it results from millenary experience and the adequate use of intelligence based on doing good for the well-being of the whole world community. It also uses nature to heal. That is magnificent!!! Thank you so much for those sincere and warm words, which honor us greatly!! Hope to meet you soon in the near future!!
This unique logo shows what he is. The Mountain (Thorax diaphragms) is Illimani (6,432m), caressing the city of La Paz, Bolivia (3,100-4,100m). The lung at high altitude, above the mountain shown with a barometer with low levels of oxygen: Hypoxia…… (art by Katia Ardaya-Zubieta).
PROF. DR. GUSTAVO ZUBIETA-CALLEJA, M.D., FPVRI The HYPOXIA MAN (India 2017) Head High Altitude Pulmonary and Pathology Institute (HAPPI-IPPA) located in La Paz, Bolivia (3,100-4,100m) in the heart of South America. Cel (591-73258026) gzubietajr@altitudeclinic.com Av. Copacabana – Prolongación # 55 Teleféricos Celeste y Blanco Av. Del Poeta, La Paz, Bolivia
Carries out joint research with his daughter Dr. Natalia Zubieta-DeUrioste, MD. They collaborate with BLDE University India, Laval University, Canada.
BUT, WHO IS HE REALLY?
……. Well… kind of difficult to say. He has been described as a “Renaissance Man” along with his father Prof. Dr. Gustavo Zubieta-Castillo, because of his extensive know-how.
He constructed with his father Prof. Dr. Gustavo Zubieta-Calleja the Chacaltaya Glass Pyramid Laboratory at 5,260masl, the highest laboratory in the world.
He has been invited to give talks in many parts of the world, including: India (5 times) USA Italy Ukraine Russia Spain Germany Poland Denmark Czech Republic Ecuador Colombia Brazil Chile Japan Tibet China
And many more…
Interested in learning more about him? Go to his blog. Make sure you navigate all around.
He constructed pulmonary function equipment, protein electrophoresis equipment, and even an elevator.
He is a top self-taught mechanical electronics engineer.
He developed hardware, software for medical records and on-line data loggers since 1981, being the first to have databases in the medical field.
Distinctions and Awards: Several, but he is not interested. Rather, he created the “Science, Honor and Truth” Award
His publications are extensively read:
Publications by Prof. Dr. Gustavo Zubieta-Calleja ordered by date.
[1] Zubieta-Castillo G, Zubieta-Calleja R, Zubieta-Calleja G. Estudios sobre la circulacion coronaria en la altura. Acta de las Primeras Jornandas de Medicina y Cirugia de la Altura; 1978 4 – 7 de Octubre La Oroya, Peru; 1978. [2] Zubieta-Castillo G, Zubieta-Calleja, G. & Zubieta-Calleja, R. El consumo de oxigeno en miocardio de perros a 3600 mt y a differentes tensiones de oxigeno. Acta de las primeras Jornadas de Medicina y Cirugia de la altura. La Oroya, Peru 1978. [3] Zubieta-Calleja G, Zubieta-Castillo, G., Zubieta-Calleja, R. La Produccion de anhidrido carbonico durante el consumo de oxigeno en miocardio de perros a 3600 m. (Abstracto). Primer Congreso Boliviano de Biología; 1979 1979; UMSS Cochabamba; 1979. [4] Zubieta-Castillo G, Zubieta-Calleja, R., Zubieta-Calleja, G. Clasificacion de la eritrocitosis en la altura de acuerdo al numero de eritrocitos (Abstracto). Primer Congreso Boliviano de Biología; 1979; UMSS Cochabamba; 1979. [5] Zubieta-Castillo G, Zubieta-Calleja GR. Chronic mountain sickness and miners (Spanish). Revista de la Academia Nacional de Ciencias de Bolivia. 1985;4:109-16. [6] Zubieta-Castillo G, Zubieta-Calleja GR. El mal de Montaña Cronico y los mineros. (Chronic mountain sickness and miners). Cuadernos Academia Nacional de Ciencias de Bolivia. 1985;62:109-16. [7] Zubieta-Castillo G, Zubieta-Calleja GR. Pulmonary diseases and chronic mountain sickness (Spanish). Revista de la Academia Nacional de Ciencias de Bolivia. 1986;5:47-54. [8] Zubieta-Castillo G, Zubieta-Calleja GR. Las Enfermedades pulmonares y el Mal de Montaña Cronico. (Pulmonary diseases and chronic mountain sickness). Cuadernos de la Academia Nacional de Ciencias de Bolivia. 1986;68:3-12. [9] Zubieta-Castillo G, Zubieta-Calleja GR. The triple hypoxia syndrome at altitude (Abstract). Amer Rev of Respir Dis. 1988;137(4):509. [10] Zubieta-Castillo G, Zubieta-Calleja GR. Iatrogenic Disease in a polycythemic patient at altitude. Amer Rev of Respir Dis. 1988;137(4):509. [11] Zubieta-Calleja GR, Zubieta-Castillo G. High Altitude Pathology at 12000 ft. La Paz: Publisher: Papiro, 1989. La Paz, Bolivia [12] Zubieta-Castillo G, Zubieta-Calleja GR. Progressive high altitude hypoventilation reversed by hyperoxia. Amer Rev of Respir Dis. 1990;141(4):a924. [13] Zubieta-Castillo. G & Zubieta-Calleja G. Hematocrit, PaO2 and PaCO2 changes in a High altitude increased Polycythemic during a 12 year follow up. Amer Rev of Respir Dis. 1990;141(4):a921. [14] Zubieta-Castillo G, Zubieta-Calleja, G & Zubieta-Calleja, L. Cambios en la PaO2, PaCO2 y el hematocrito en un paciente con mal de montaña cronico durante 12 años. Acta del Quinto Congreso Nacional de Medicina de la Altura; 1992; La Oroya, Peru; 1992. p. 136. [15] Zubieta-Castillo G, Zubieta-Calleja G. Acute Hypoventilation on ascent to high altitude. European Respiratory Society Congress; 1992; Vienna, Austria; 1992. [16] Zubieta-Castillo G, Zubieta-Calleja GR. El Sindrome de Triple Hipoxia en la Altura. Acta del Quinto Congreso Nacional de Medicina de la Altura; 1992; La Oroya, Peru; 1992. p. 136. [17] Zubieta-Castillo G, Zubieta-Calleja G. Eritrocitosis agudas, EPOC y sindrome de triple hipoxia. Acta del Quinto Congreso Nacional de Medicina de la Altura; 1992; La Oroya, Peru; 1992. p. 135. [18] Zubieta-Calleja G, Zubieta-Castillo G. High altitude illness in Bolivia (Abstract). First World Congress of High Altitude Medicine and Physiology; 1994; La Paz, Bolivia: Edvil;p. 58.
[20] Zubieta-Calleja GRZ-C, G and Zubieta-Calleja, L. Zubieta-Calleja, G.R. Zubieta-Castillo, G and Zubieta-Calleja, L.. Inadequate treatment of excessive erythrocytosis. Acta Andina. 1995;4:123-6. [21] Zubieta-Calleja GZ-C, G. Chronic Mountain Scikness. Proceedings of the Third Symposium on High Altitude Medicine and Physiology; 1995; Xining, Gingai, PR China; 1995. p. 40. [22] Triplett J, Zubieta-Calleja L, Zubieta-Castillo G, Zubieta-Calleja GR. Physiological changes related to rapid altitude shifts in La Paz, Bolivia. Acta Andina. 1996;5(1):19-21. [23] Zubieta-Calleja GR, Zubieta-Castillo G. High Altitude Pathology Institute. 1996 [cited 2007 june 15, 2007]; Available from: http://www.altitudeclinic.com [24] Zubieta-Calleja G. and Zubieta-Castillo GR. International Soccer vetoed in Stadiums above 3000 m of altitude. International Society for Mountain Medicine. 1996;6(1). [25] Zubieta-Calleja GR, Zubieta-Castillo, G and Zubieta-Calleja, L. Can HAPE be diagnosed through the tongue? Acta Andina. 1996;5:31-4. [26] Zubieta-Castillo G, Zubieta-Calleja G. Triple hypoxia syndrome. Acta Andina. 1996;5(1):15-8. [27] Zubieta-Castillo G, Zubieta-Calleja G. New Concepts on chronic mountain sickness. Acta Andina. 1996;5:3-8. [28] Zubieta-Calleja G, De Urioste, L. & Zubieta-Calleja, L. High altitude residents in Bolivia. Progress in Mountain Medicine and High Altitude Physiology. In: HidekiOhno TK, Shigeru Masuyama and Michiro, Nakashima, ed. Progress in Mountain Medicine and High Altitude Physiology. Matsumoto, Japan 1998:185-9. [29] Zubieta-Calleja G, Zubieta-Castillo G. Changes in oximetry during breath holding in normal residents of high altitude. In: Hideki Ohno TK, Shigeru Masuyama and Michiro, ed. Progress in Mountain Medicine and High Altitude Physiology. Matsumoto, Japan 1998:343-8. [30] Zubieta-Castillo G, Zubieta-Calleja G, Arano E, Zubieta-Calleja L. Respiratory Disease, chronic mountain sickness and gender differences at high altitude. In: HidekiOhno TK, Shigeru Masuyama and Michiro, Nakashima., ed. Progress in Mountain Medicine and High Altitude Physiology. HidekiOhno, Toshio Kobayashi, Shigeru Masuyama and Michiro, Nakashima. 1998:132-7. [31] Zubieta-Castillo G, Zubieta-Calleja GR. Pulse oximetry in chronic mountain sickness- long breath holding time and oscillation at lowest saturation. In: HidekiOhno TK, Shigeru Masuyama and Michiro, Nakashima, ed. Progress in Mountain Medicine and High Altitude Physiology 1998:349-54. [32] Pollard AJ, Niermeyer S, Barry P, Bartsch P, Berghold F, Bishop RA, et al. Children at high altitude: an international consensus statement by an ad hoc committee of the International Society for Mountain Medicine, March 12, 2001. High Alt Med Biol. 2001 Fall;2(3):389-403. [33] Zubieta-Calleja G, Zubieta-Castillo, G., Zubieta-Calleja, L. & Zubieta, N. Exercise performance of bolivian aymara in 3 conditions: at La Paz 3,510 m, breathing a hypoxic mixture simulating Chacaltaya and at Chacaltaya 5,200 m. HAMB. 2002;3(1):114-5. [34] Zubieta-Calleja G, Zubieta-Castillo, G., Zubieta-Calleja, L., Zubieta, N. Measurement of circulatory time using pulse oximetry during breath holding in chronic hypoxia. HAMB. 2002;3(1):115. [35] Zubieta-Calleja GR, Zubieta-Castillo, G., Zubieta-Calleja, L., Zubieta, N. Breath holding and pulse oximetry as a diagnostic tool at high altitude. HAMB. 2002;3(1):115. [36] Zubieta-Calleja GR, Zubieta-Castillo, G., Zubieta-Calleja, L., Zubieta, N. Exercise performance in chronic mountain sickness (cms) patients at 3510 m. HAMB. 2002;3(1):114-5. [37] Zubieta-Castillo G, Zubieta-Calleja, G.R., Zubieta-Calleja, L. Exercise performance in a woman with CMS following triple hypoxia syndrome treatment. HAMB. 2002;3(1):114-5. [38] Zubieta-Castillo G, Zubieta-Calleja, G.R., Zubieta-Calleja, L., Zubieta, N. Bolivian Aymara that played soccer at 6542 m maintain higher oxygen saturation and lower oxygen uptake during maximal exercise. HAMB. 2002;3(1):114-5. [39] Zubieta-Castillo G, Zubieta-Calleja GR, Zubieta-Calleja L, Zubieta C, Nancy. Adaptation to life at the altitude of the summit of Everest. Fiziol Zh. 2003;49(3):110-7. [40] Zubieta-Calleja (Jr) GR, Moretti M, Zubieta-Calleja L, Zubieta N, Zubieta-Castillo (Sr) G. Chronic mountain sickness among the Chipaya after 2500 years of high altitude exposure. HAMB. 2004;5(2):291-2. [41] Zubieta-Calleja (Jr) GR, Zubieta-Castillo (Sr) G, Zubieta-Calleja L, Zubieta N. Hypoventilation in Chronic Mountain Sickness: a mechanism to preserve energy. HAMB. 2004;5(2):291-2. [42] Zubieta-Calleja G. Bloodletting: a medical resource since the stone age. Journal of Qinghai Medical College. 2004;25(4):273-5. [43] Zubieta-Castillo (Sr) G, Zubieta-Calleja (Jr) GR, Zubieta-Calleja L, Zubieta N. How chronic mountain sickness (cms) contributed to the theory of life at the hypoxic levels of the summit of Mount Everest. HAMB. 2004;5(2):291-2. [44] Fabiola León-Velarde, Marco Maggiorini, John T Reeves, Almaz Aldashev, Ingrid Asmus, Luciano Bernardi, Ri-Li Ge, Peter Hackett, Toshio Kobayashi, Lorna G Moore, Dante Penaloza, Jean-Paul Richalet, Robert Roach, Tianyi Wu, Enrique Vargas, Gustavo Zubieta-Castillo, Gustavo Zubieta-Calleja. Consensus statement on chronic and subacute high altitude diseases. High Alt Med Biol. 2005 Summer;6(2):147-57. [45] Paulev PE, Zubieta-Calleja GR. Essentials in the diagnosis of acid-base disorders and their high altitude application. J Physiol Pharmacol. 2005 Sep;56 Suppl 4:155-70. [46] Zubieta-Calleja GR, Zubieta-Castillo G, Paulev PE, Zubieta-Calleja L. Non-invasive measurement of circulation time using pulse oximetry during breath holding in chronic hypoxia. J Physiol Pharmacol. 2005 Sep;56 Suppl 4:251-6. [47] Zubieta-Calleja GR, Paulev PE, Zubieta-Calleja L, Zubieta-Calleja N, Zubieta-Castillo G. Hypoventilation in chronic mountain sickness: a mechanism to preserve energy. J Physiol Pharmacol. 2006 Sep;57 Suppl 4:425-30. [48] Zubieta-Calleja GR, Zubieta-Castillo G, Zubieta-Calleja L, Zubieta N. The increase in hematocrit during the high altitude adaptation process. (Abstract). Wilderness Environ Med. 2006 Fall;17(3):202-3. [49] Zubieta-Castillo G, Sr., Zubieta-Calleja GR, Jr., Zubieta-Calleja L. Chronic mountain sickness: the reaction of physical disorders to chronic hypoxia. J Physiol Pharmacol. 2006 Sep;57 Suppl 4(2):431-42. [50] Paulev P-E, Zubieta-Calleja G. High Altitude Diving Depths. Res in Sports Med. 2007;15(1 or 2 in print). [51] Zubieta-Calleja GR, Paulev P-E, Zubieta-Calleja L, Zubieta-Castillo G. Altitude adaptation through hematocrit changes. J of Physiol and Pharmacol. 2007;58(Supplement). [52] Zubieta-Castillo G, Zubieta-Calleja GR. Facts that Prove that Adaptation to Life atExtreme Altitude (8848m) is Possible. In: L.Lukyanova NTaPKS, editor. Adaptation Biology and Medicine: Health Potentials; 2007; New Dehli, India: Narossa Publishing House; 2007. [53] Gustavo Zubieta-Calleja GZC, Poul-Erik Paulev (2009) The Adaptation of Highlanders to Sea Level. In Wilderness & Environmental Medicine- Wilderness Conference and Annual Meeting. (ed.), Vol. 20, pp. 184-5, Wilderness & Environmental Medicine-Official Publication of the Wilderness Medical Society, Snowmass, Colorado. [54] Zubieta-Calleja G, Zubieta-Castillo G, Zubieta-Calleja L, Ardaya-Zubieta G, and Paulev PE (2009) Do over 200 million healthy altitude residents really suffer from chronic Acid-Base disorders? Indian J Clin Biochem 26, 62-5. [55] Zubieta-Calleja L (2009) The High Altitude Adaptation Formula. In 36th Annual Conference of Association of Clinical Biochemists of India. (ed.), Vol. 24, pp. 83-4, Indian Journal of Clinical Biochemistry- Association of Clinical Biochemists of India, Kochi, India. [56] Zubieta-Castillo G (2012) Loss of Adaptation and Maladaptation: two terms Inadequately used-Conversely-“Adaptation: A Fundamental Law of Biology that at High Altitude, even Permits Life at the Hypoxic Levels of Mt. Everest”. In Global Hypoxia Summit & 4th International Conference on Chr onic Hypoxia. (ed.), Vol. pp. 74-5, New Delhi, India. [57] Zubieta-Calleja, G, Zubieta-Castillo, G, Merishi, J. (2012) Extremely high altitude hypoxic conditions during Mount Everest expeditions, residence at South Pole stations, in Tibet and among the Andes: Van Slyke equation modification is crucially important for acid–base measurements. Journal of Biological Physics and Biochemistry 12(3):103-112. [58] Balaban DY, Duffin J, Preiss D, Mardimae A, Vesely A, Slessarev M, ZubietaCalleja G, et al.(2013) The in-vivo oxyhaemoglobin dissociation curve at sea level and high altitude. Respir Physiol Neurobiol 186, 45-52. [59] Zubieta-Calleja, GR, Ardaya, G, Zubieta-DeUrioste, N, Paulev, PE, Zubieta-Castillo, G. Tolerance to Hypoxia (2013) Vol 59:4 Fiziol Journal. Kiev, Ukraine. [60] Zubieta-Castillo, G and Zubieta-Calleja GR.(2014) High Altitude Research and its Clinical Application. Chapter in Book Translational Research in Environmental and Occupational Stress. Editors: Chachi Bala Singh, Nanduri R. Prabhakar, Crinivas N. Pentyala. Springer India. [61] Zubieta-Calleja GR, Zubieta-DeUrioste NA. Extended longevity at high altitude: Benefits of exposure to chronic hypoxia. BLDE Univ J Health Sci 2017;2:80-90 [62] Zubieta-Calleja, G.R.; Zubieta-DeUrioste, N.; Venkatesh, T.; Das, K.; Soliz, J. COVID19: Multiple Diseases Simulating Extreme High-Altitude Exposure? Oxygen Transport Physiology and Scarce Need of Ventilators; Andean Condor’s-Eye-View. Preprints 2020, 2020050085 (doi: 10.20944/preprints202005.0085.v1). [63] Zubieta-Calleja, G., & Zubieta-DeUrioste, N. (2020, September 27). Pneumolysis and “silent hypoxemia” in COVID-19. https://doi.org/10.31219/osf.io/qde8w [64] Roberto Carlos Vera, Natalia Zubieta-DeUrioste, Gustavo Zubieta-Calleja, (Oct 2020) La quema de los bosques bolivianos afecta la calidad del aire y atenta contra la salud en estos tiempos de pandemia COVID- https://zuniv.net/pub/BOLET%C3%8DN1Ambiente_13oct.pdf. [65] Arias-Reyes C, Zubieta-DeUrioste N, Poma-Machicao L, Aliaga-Raduan F, CarvajalRodriguez F, Dutschmann M, Schneider-Gasser EM, Zubieta-Calleja G, Soliz J. Does the pathogenesis of SARS-CoV-2 virus decrease at high-altitude? Respir Physiol Neurobiol. 2020 Jun;277:103443. doi: 10.1016/j.resp.2020.103443. Epub 2020 Apr 22. PMID: 32333993; PMCID: PMC7175867. [66] Soliz J, Schneider-Gasser EM, Arias-Reyes C, Aliaga-Raduan F, Poma-Machicao L, Zubieta-Calleja G, Furuya WI, Trevizan-Baú P, Dhingra RR, Dutschmann M. Coping with hypoxemia: Could erythropoietin (EPO) be an adjuvant treatment of COVID-19? Respir Physiol Neurobiol. 2020 Aug;279:103476. doi: 10.1016/j.resp.2020.103476. Epub 2020 Jun 6. PMID: 32522574; PMCID: PMC7275159. [67] Gustavo R. Zubieta-Calleja*, Natalia Zubieta-DeUrioste, Thuppil Venkatesh, Kusal K. Das and Jorge Soliz, “COVID-19 and Pneumolysis Simulating Extreme High-altitude Exposure with Altered Oxygen Transport Physiology; Multiple Diseases, and Scarce Need of Ventilators: Andean Condor’s-eye-view”, Reviews on Recent Clinical Trials (2020) 15:
https://doi.org/10.2174/1574887115666200925141108 [68] Zubieta-Calleja, G., Merino-Luna, A., Zubieta-DeUrioste, N., Armijo-Subieta, NF., Soliz, J., Arias-Reyes, C. , Escalante-Kanashiro, R., Carmona-Suazo, J., López-Bascope, A., Calle-Aracena, J., Epstein, M. & Maravi, E (2020, October 15). COVID-19 patients in the high-altitude areas of Bolivia and Peru manifest a substantive decrease in mortality. https://doi.org/10.31219/osf.io/7rd2h [69] Zubieta-Calleja G, Zubieta-DeUrioste N. Pneumolysis and “Silent Hypoxemia” in COVID-19. Indian J Clin Biochem. 2020 Nov 9;36(1):1-5. doi: 10.1007/s12291-020-00935-0. Epub ahead of print. PMID: 33191989; PMCID: PMC7652053. [70] Zubieta-Calleja G, Merino-Luna A, Zubieta-DeUrioste N, Armijo-Subieta NF, Soliz J, Arias-Reyes C, Escalante-Kanashiro R, Carmona-Suazo JA, López-Bascope A, Calle-Aracena JM, Epstein M, Maravi E. Re: “Mortality Attributed to COVID-19 in High-Altitude Populations” by Woolcott and Bergman. High Alt Med Biol. 2021 Feb 9. doi: 10.1089/ham.2020.0195. Epub ahead of print. PMID: 33567217. [71] Zubieta-Calleja G, Zubieta-DeUrioste N. Acute Mountain Sickness, High Altitude Pulmonary Edema, and High Altitude Cerebral Edema: A view from the High Andes. Respir Physiol Neurobiol. 2021 Feb 2;287:103628. doi: 10.1016/j.resp.2021.103628. Epub ahead of print. PMID: 33545376. [72] Zubieta-Calleja G, Zubieta-DeUrioste N. The Oxygen Transport Triad in High-Altitude Pulmonary Edema: A Perspective from the High Andes. International Journal of Environmental Research and Public Health. 2021; 18(14):7619. https://doi.org/10.3390/ijerph18147619
Much to many world scientists’ surprise, a group of sea-level “International high altitude experts” who defend a different point of view, wrote to the Chief Editor of the prestigious journal Respiratory Physiology and Neurobiology questioning our article: “Acute Mountain Sickness, High Altitude Pulmonary Edema, and High Altitude Cerebral Edema: A view from the High Andes” by Prof. Dr. Gustavo Zubieta-Calleja [his CV] and Dr. Natalia Zubieta-DeUrioste, published in Volume 287, May 2021 of the Respiratory Physiology & Neurobiology. Available as a Pre-print here. A full Journal printed scan version is available on request from the authors. Please send us an email.
full version copy available on request from authors at gzubietajr@gmail.com
Interestingly, the same article received multiple congratulations and support. Simultaneously, the prestigious International Journal of Environmental Research and Public Health with an Impact Factor of 3.3 asked the author for an extension of the paper. Consequently, “The Oxygen Transport Triad in High-Altitude Pulmonary Edema: A Perspective from the High Andes” was published. In it, several of the questions are addressed.
Many scientists from around the world are giving their support asking for a NO RETRACTION of the paper, as any questioning should follow a standard course through a Letter to the Editor.
Some comments of support by very distinguished scientists of include:
Dear Gustavo You have taken the right step for world scholars’ opinion to the journal. I am always with you and will be. It is disgusting to see some Western scientists’ attitudes towards Latin America and South Asian community fellow colleagues. Science always prevails with experience, observation, and truth. Yes I agree that nothing is a universal truth in science and that is the beauty of science but ‘what I think is always right and there will not be any “alternate hypothesis” is a shallow mindset of a few people who never tested their own hypothesis in other environments. Your research and honesty are beyond any doubt. You are not only a great scientist but also a great physician with credibility. I did not find anything wrong or unscientific in this interesting thought-provoking research article with facts and deep logical analysis. To me, it is a great Science and I shall teach your alternate but strong theories and explanations to my University students without hesitations as a great novel contribution of high altitude biology. I believe your work is a part of the progress of science for serving humanity!
I not only oppose the idea of this great publication retraction but also condemn it.
Regards
Kusal K.Das, PhD, FRSB Distinguished Chair Professor in Vascular Physiology Laboratory of Vacular Physiogy and Medicine Faculty of Medicine BLDE ( Deemed to be University ), Vijayapur, Karnataka, India (560m) Former Vising Professor School of Medicine University of Leeds, UK ( 2014 – 2016 ) Hony.Fellow Karnataka Academy of Science & Technogy Government of Karnataka President South Asian Association of Physiologists ( HO. University of Colombo ). President’s message, above. Member of International Union of Physiological Sciences (IUPS) IUPS is the world body of physiologists with 84 countries and hundred societies
Dear Gustavo, I fully support your publication. My details are as follows.
Prof. Praveen Sharma PhD (Med), FACBI, FAMS, FAACC Professor of Biochemistry, (Former Head Biochemistry, Dean (Research) & Controller of Examinations), All India Institute of Medical Sciences, Jodhpur-342005 ( India) President ACBI (2003-2004 and 2014-2015) President, InSLAR (2017 to date) Chair, IFCC-CCLM (2020-to date) Director, South East Asia on WASPaLM Board (2021 to date) Editor-in-Chief, IJCB (2006 to date), Chairman, APFCB Congress and Conferences (2019 to date) Chairman, APFCB Communication committee (2010-2019) Chief Editor, APFCB News (2010-2019) Director, NRCLPI, Jodhpur (2014 to date) Assessor (NABL ) International Lead Assessor (AERSSC) Mobile:+91-8003996869 +91-9414044562 Email: praveensharma55@gmail.com sharmapr@aiimsjodhpur.edu.in
Someone has to pioneer the road to higher consciousness through scientific exploration. You have. Your paper is stellar and ahead of its time. There was a saying in the 1960s I abide by: “keep on keeping on.” Be proud of your forward-thinking ideals. Westerners will catch up to you in time.
Dr. Kathryn Rossie, PhD Clinical Psychologist Researcher Author, Publisher, and Editor Consultant: International level. Private Practice Consultation: California. Professor of the Neuroscience Institute for Psychotherapists of San Lorenzo Maggiore, Italy. Chief Financial Officer (CFO) and Vice President: The Ernest Lawrence Rossi Non-Profit Foundation for Psychosocial Genomics Research Board of Directors: The Milton H. Erickson Foundation Press Founding Director of the Milton H. Erickson Institue of the California Central Coast (MHE-CCC)
All high altitude researchers in India including HPRC (High Altitude Physiology Research Cell, Darjeeling), high altitude research facilities St John’s team, Defense Institute of Physiology and Allied Sciences (DIPAS) are all in support of the research paper published by Professor Gustavo et al. We require scientific community to take this concept forward without any bias and come out with the most appropriate guidance documents to manage chronic Hypoxia. With regards,
Dr Thuppil Venkatesh President International Society of Chronic Hypoxia CEO and Director Chairman Indian Society for Lead awareness and research and Director The National Referral Center for Lead Poisoning Prevention in India (NRCLPI) Foundation for Quality India (FQI) The Lead Man of India Professor Emeritus Biochemistry Department St John’s Medical College Bangalore, India
Dear Gustavo,
Thank you for the materials you sent me. I need some time to study these materials more closely, delving into the arguments and comparing them.
Being a specialist in some intracellular molecular mechanisms of adaptation to hypoxia, I will not take the responsibility to take part in the discussion on issues of respiratory physiology and practical medicine.
However, in any case, I consider the precedent of retraction of the already published article extremely dangerous. This not only destroys constructive scientific discussion, based on the freedom of publication by each of the side of its position and arguments. This also threatens us with an Orwellian dystopia of an unpredictable changing past. This precedent is especially dangerous in conditions when more and more scientific journals have only an electronic version and are not published in paper form. With this approach, we can get a situation where, with each change of the prevailing concepts in science, articles previously published in electronic journals will “disappear” as if they never existed.
Of course, I join to letter to the Chief Editor and Publishers asking for NO RETRACTION.
Sincerely,
Dr. Sergei Alexandrovich Stroev, PhD I.P. Pavlov Institute of Physiology of Russian Academy of Sciences, Russia (2000-2015), University of Tampere, School of Medicine, Finland (2001-2014).
P.S. By the way, I was somewhat surprised by point 4 of your opponents’ objections, where they state: «“adaptation” must be limited to genetically transmissible changes because they are integrated into the gene pool of a particular population or species».
My thesis, which I successfully defended in University of Tampere was called “The role of endogenous protein antioxidants in neuronal adaptation to hypobaric hypoxia”.
The dissertation dealt with adaptation to hypoxia of cells and the organism as a whole at the level of regulation of the expression of individual proteins without any genetically transmissible changes (I will not vouch for epigenetic changes in this model – I have not studied this issue). And the term “adaptation” in this sense of an individual, not related to genetic changes, adaptation did not cause any objections from highly professional opponent, reviewers and many specialists who were present at the defense of the thesis.
Many other authors use this term in the same meaning, for example:
Samoilov M.O. Brain and adaptation. Molecular and cellular mechanisms. St. Petersburg,
Continuous adaptation of rats to hypobaric hypoxia prevents stressor hyperglycemia and optimizes mitochondrial respiration under acute hypoxia. Fiziol Zh. 2012 b. 58(5): 56-64 (In Ukrainian, summary in English).
Meerson F., Pozharov V., Minyailenko T. Superresistance against hypoxia after
Lukyanova L.D., Sukoyan G.V., Kirova Y.I. Role of proinflammatory factors, nitric
oxide, and some parameters of lipid metabolism in the development of immediate adaptation to hypoxia and HIF-1α accumulation. Bull Exp Biol Med. 2013. 154(5): 597-601.
Lu G., Ding D., Shi M. Acute adaptation of mice to hypoxic hypoxia. Biol Signals Recept. 1999. 8(4-5): 247-255.
49 world distinguished scientists have supported the quality of this article. We are most thankful !
We also have great support from a growing number of people 1,789 as of Aug 20, 2021 that also support our article.
The original article was printed in the Volume 287, May 2021 of the Respiratory Physiology and Neurobiology journal
We have just published our latest enhanced version in the top level Journal Reviews on Environmental Health, responding to the observations made by those 17 “sea level high-altitude experts”.
As everyone on the planet knows, the coronavirus has attacked in a fierce way, due to its high speed of contagion and its physical characteristics. The advanced countries of the first world have suffered the impact in an alarming way. And they are fighting an almost uncontrollable battle.
In Bolivia, the Government has correctly made rapid quarantine decisions, which constitute an essential measure in order to avoid the subsequent overload of medical centers and especially intensive care units, which are very limited.
This is not an easy measure to carry out and understand in its complexity, but it is a fundamental defense mechanism to flatten the incidence curve. That is, instead of being initially exponential or hyperexponential (as I have called it, because it does not double every time, but one person can infect many at once), shooting upwards, it becomes a flattened quasi-logarithmic progression. In other words, a mathematical change occurs, very important in its evolution.
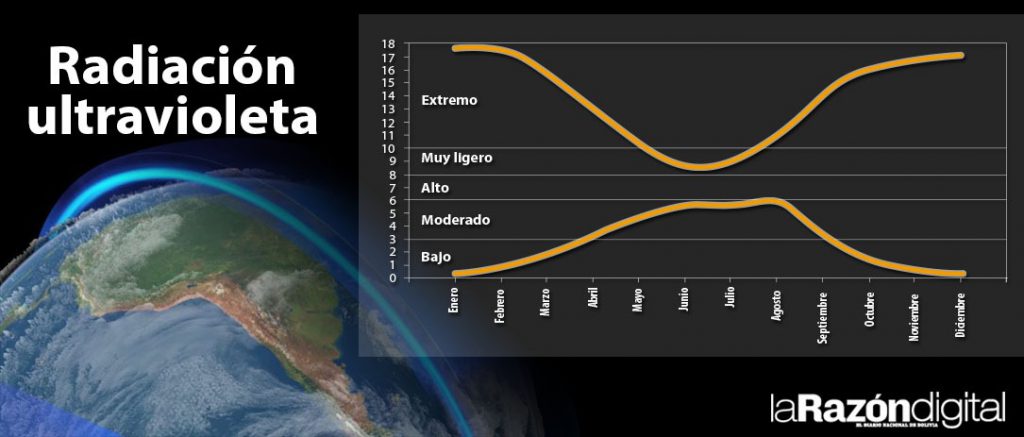
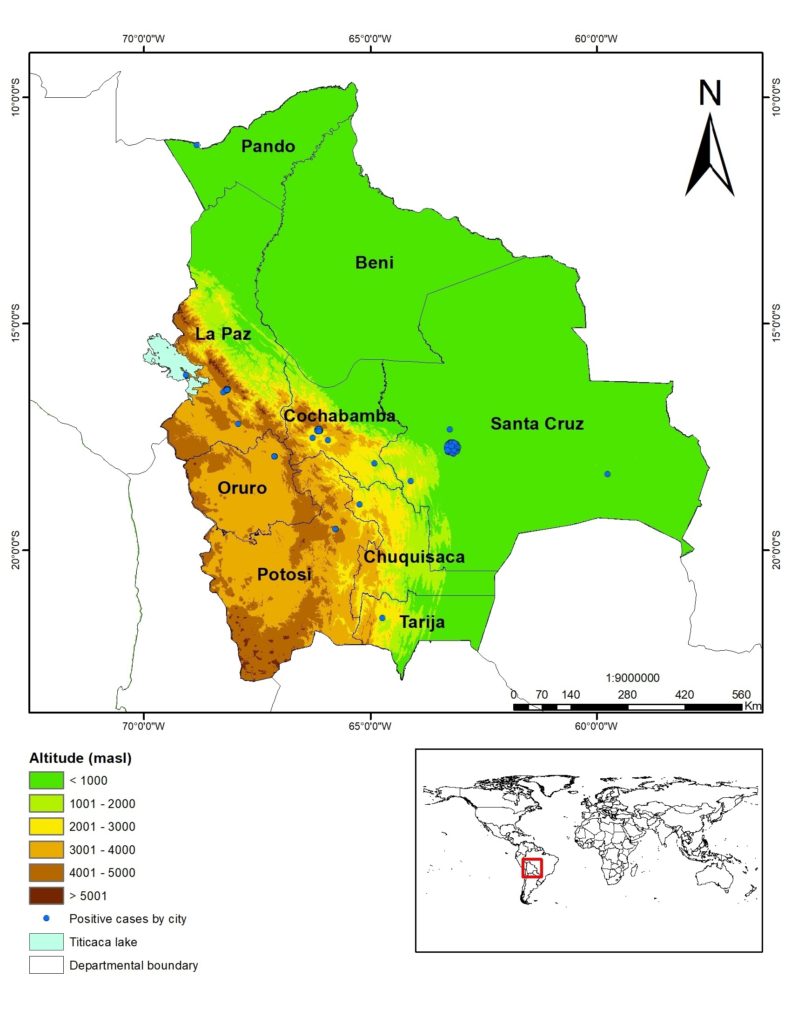
Ultra-violet radiation, a component of light that comes from the sun, is very strong at high altitudes in cities above 3,000 meters above sea level (especially) such as La Paz (3,100-4,100), El Alto (4000-4100), Oruro (3,800) and Potosí (4,000), in Bolivia.
The ultraviolet radiation index (UVindex) is considered to be at extreme levels in La Paz, as we found in a publication with Danish colleagues more than 10 years ago in the following graph, where the top line is La Paz, Bolivia 3,600, and the bottom Copenhagen, Denmark
Radiacion Ultravioleta
Footnote: Kessel, L., Kofoed, PC, Zubieta-Calleja, GR & Larsen, M. Acta Opthalmologica.88 (2): 235-40, March 2009.
As an expert in altitude medicine, I was invited by Prof. Kusal Das to participate in the UNESCO International Forum on COVID-19 with Chairman Prof. Sinerik Ayrapetyan, on Friday, March 27.
Various experts spoke about the molecular characteristics of the coronavirus, of the incidences in their countries, such as Italy, the United States, India and Iran, among others. The mechanisms of action of the virus were analyzed and the search for different treatment techniques was discussed, taking into account many characteristics of the virus.
Next I expose part of what I exposed:
1) Ultraviolet radiation is a protection factor against this virus, because it is lethal. One of the ways the disease is transmitted is because it sits on surfaces where it stays alive for several hours and possibly even days.
But at high-altitude, solar radiation constitutes a sterilizer of all surfaces where the sun falls. That is why the streets in high-altitude cities benefit from this physical characteristic. As an expert, I always said that ultraviolet radiation was beneficial.
Of course, some are afraid of sun exposure because it could lead to skin cancer, but there are no systematic studies to prove these claims. The body adapts to the highest levels of radiation; otherwise people living in the highlands would have a high incidence of cancer, from a long time ago and nowadays.
Quite the contrary, ultraviolet radiation is now a formidable mechanism for our defense against the virus.
2) Dr. Jorge Solíz, from Laval University, Canada, also observed that in China there were no cases or they were very rare in the Tibet area. Together with other colleagues we are writing a scientific article on this topic. Dr. Kusal Das, from BLDE University, in India, where I am a “visiting professor”, likewise noted that there is lower incidence in high altitude areas in his country.
3) In December 2018 we published with my collaborator Dr. Natalia Zubieta de Urioste an article in relation to the advantages of life at high-altitude, in which we affirm that man lives longer at high-altitude.
We demonstrate this with a longevity graph in all Bolivian cities (based on Segip , local citizen registration office, data), which shows an upward curve starting in Pando at 300m and ending in Potosí at 4100m. In it we also mention the advantages of ultraviolet radiation at high-altitude.
4) Ultraviolet lights are currently being built for use in hospitals and intensive care rooms. Even a Bolivian company in Santa Cruz, whom I congratulate.
5) The low incidence of infections in Oruro, undoubtedly, is due to a strict quarantine (if I’m not mistaken, the first in the country). It deserves our recognition because at the moment the initial eight cases have not increased, with only “patient zero” is an imported case in Oruro).
But I must add that ultraviolet radiation, our ally in high-altitude cities, is also playing an important role. This does not mean, however, that other cases may not appear eventually, because there are many variables, but at the end of this pandemic the statistics will most likely show thatat high-altitude there was a lower incidence.
This does not mean, however, that you must let your guard down. There are also other technical aspects of adaptation to height that we will mention very shortly.
6) On January 30, 2020, in an interview with University Radio-Tv, thanks to a kind invitation from Johnny Villarroel, who directs the Disarmed Discourse program, in which Gonzalo Taboada, president of the Bolivian Academy of Sciences also participated , I stated the following:
That coronavirus treatment centers, with intensive care rooms, should be installed in remote and isolated areas of the cities so as to avoid contamination. I recommended that patients not be taken to centrally located hospitals, leaving them free to care for common illnesses.
In the case of La Paz, I suggested that it be in the highlands, precisely because there is more ultraviolet radiation there. But I also made a recommendation: subsequently, intensive therapy treatment rooms should have a partially glass ceiling, like skylights, to allow ultraviolet light to enter, in order to sterilize the environment in a natural way.
Hopefully in the future the importance of these suggestions will be understood.
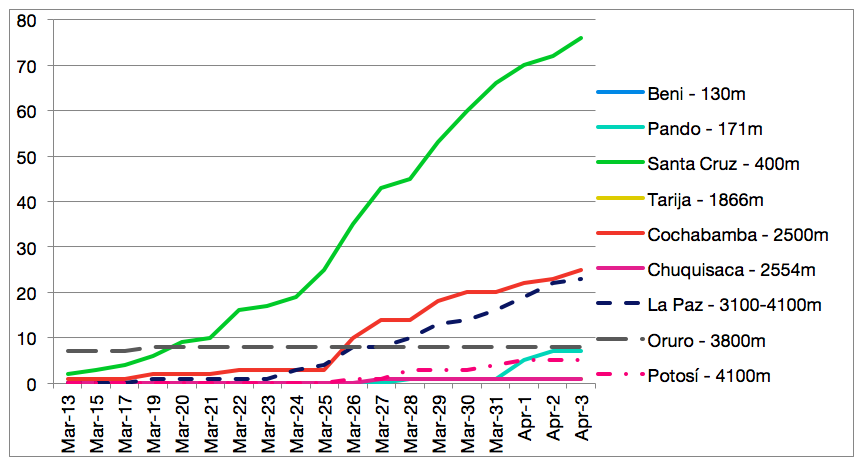
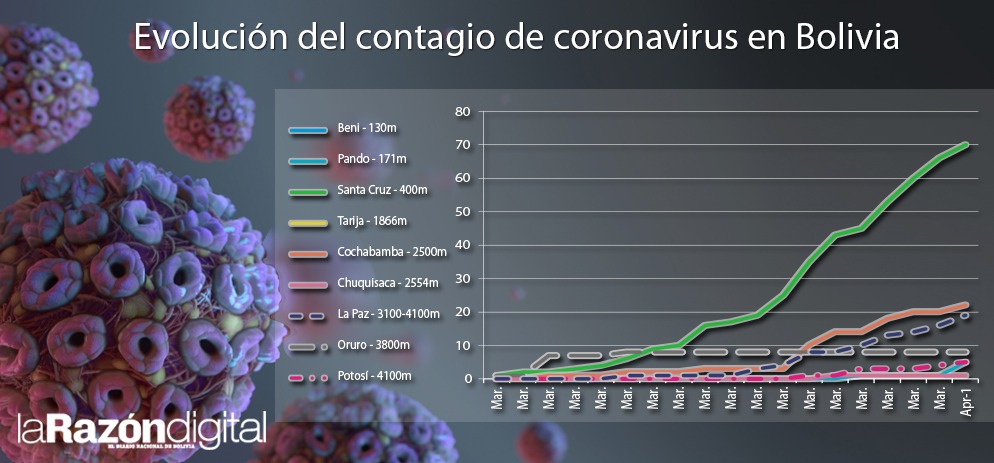
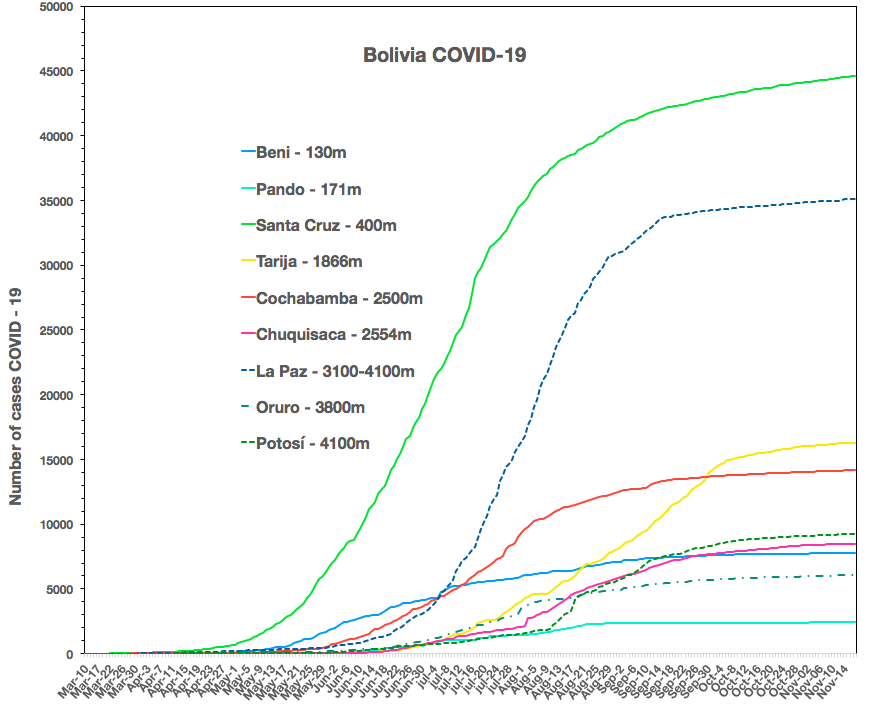
7) The following graph shows the evolution of coronavirus infections in Bolivia in which it is clearly observed that in high-altitude cities (with broken lines) there is less incidence as a function of time:
8) It is also recommended that when someone arrives at home and takes off the clothes used on the street, they should expose them to the sun during this stage. This will allow the virus to be removed quickly (possibly 1/2 hour).
9) It is important to mention that, as inhabitants of the highlands, if one were to suffer a very severe case of CoVid-2 that evolves favorably, thanks to the treatments of the heroic doctors, nurses and health personnel in the highland areas, the consequences of the lung lesions could leave fibrosis (scars), hindering exercise capacity.
These people would develop a Chronic Mountain Sickness (PoliEritroCitemia),in more than a month and a half, which is a compensatory mechanism against chronic respiratory insufficiency, .
Several are likely to be able to stay and develop their lives normally at high-altitude with proper medical care.
Finally, I must add that you should not let your guard down, because although there are fewer cases at altitude, there are cases, of course, and we must all respect the quarantine.
He is a doctor, professor and director of the High Altitude Pulmonary and Pathology Institute (IPPA)
Las ventajas de la radiación ultravioleta en el control del coronavirus en la altura
En Bolivia, el Gobierno ha tomado correctamente decisiones rápidas de cuarentena, que se constituyen una medida esencial a fin de evitar la sobrecarga posterior de los centros médicos y sobretodo de las unidades de terapia intensiva, que son muy limitadas
Como todos en el planeta sabemos, el coronavirus ha atacado de una forma feroz, por su gran velocidad de contagio y sus características físicas. Los países avanzados del primer mundo han sufrido el impacto de una manera alarmante. Y están librando una batalla casi incontrolable.
En Bolivia, el Gobierno ha tomado correctamente decisiones rápidas de cuarentena, que se constituyen una medida esencial a fin de evitar la sobrecarga posterior de los centros médicos y sobretodo de las unidades de terapia intensiva, que son muy limitadas.
Ésta no es una medida fácil de llevar a cabo y entenderla en su complejidad, pero es un mecanismo de defensa fundamental para aplanar la curva de incidencia. Es decir, en vez de que sea inicialmente exponencial o hiperexponencial (como la he denominado, porque no se dobla cada vez, sino una persona puede contagiar a muchos a la vez), disparándose hacia arriba, se la vuelve una progresión cuasi logarítmica aplanada.
Es decir se produce un cambio matemático, muy importante en su evolución. La radiación ultra-violeta, componente de la luz que proviene del sol, es muy fuerte en la altura en las ciudades por encima de los 3.000 msnm (sobretodo) como La Paz (3.100-4.100), El Alto (4000-4100), Oruro (3.800) y Potosí (4000), en Bolivia.
Se considera que el índice de radiación ultravioleta (UVindex) está en niveles extremos en La Paz, como lo constatamos en una publicación con unos colegas daneses hace más de 10 años en la siguiente gráfica, donde la línea delgada es La Paz, Bolivia 3.600, y la gruesa Copenhagen, Dinamarca
Pie de gráfica: Kessel, L., Kofoed, P.C., Zubieta-Calleja, G.R. & Larsen, M. Acta Opthalmologica.88(2):235-40, March 2009.
Como experto en medicina de altura fui invitado a participar en el Forum Internacional sobre COVID-19 de la UNESCO, el viernes 27 de marzo, como único exponente de toda Sudamérica.
Diversos expertos hablaron sobre las características moleculares del coronavirus, de las incidencias en sus países, como Italia, Estados Unidos, India e Irán, entre otros. Se analizaron los mecanismos de acción del virus y se discute la búsqueda de diferentes técnicas de tratamiento, tomando en cuenta muchas características del virus.
A continuación expongo parte de lo que expuse:
1) La radiación ultravioleta es un factor de protección ante este virus, porque le resulta letal. Una de las formas de transmisión de la enfermedad es porque se asienta en superficies donde se mantiene con vida durante varias horas y posiblemente hasta días.
Pero en la altura, la radiación solar se constituye en un esterilizador de toda superficie donde cae el sol. Por eso las calles en las ciudades de altura se benefician de esta característica física de la altura. Como experto, siempre dije que la radiación ultravioleta era beneficiosa.
Por supuesto que algunos tienen miedo de exponerse al sol porque podría producir cáncer de la piel, pero no existen estudios sistemáticos que prueben estas afirmaciones. El organismo se adapta a los niveles más altos de radiación; de otra manera la gente que vive en el altiplano tendría mucha incidencia de cáncer, desde antes y en la actualidad.
Al contrario, la radiación ultravioleta ahora resulta un mecanismo formidable para nuestra defensa ante el virus.
2) El doctor Jorge Solíz, de Universidad de Laval, de Canadá, también observó que en China no hubo casos o fueron muy raros en la zona del Tíbet.
En forma conjunta con otros colegas estamos escribiendo un artículo científico sobre este tema. El doctor Kusal Das, de la BLDE University, en India, donde soy “professor visitante”, también notó que en las zonas de altura en su país hay menor incidencia.
3) En diciembre de 2018 publicamos con mi colaboradora la doctora Natalia Zubieta de Urioste un artículo en relación a las ventajas de la vida en la altura, en el que afirmamos que el hombre vive más largo en la altura.
Lo demostramos con un gráfico de longevidad en todas las ciudades de Bolivia (basada en datos del Segip), que muestra una curva ascendente empezando en Pando y terminado en Potosí.
Allí también mencionamos las ventajas de la radiación ultravioleta en la altura.
4) Actualmente se están construyendo luces ultravioleta para utilizar en los hospitales y salas de terapia intensiva. Incluso una compañía boliviana en Santa Cruz, a la que felicito.
5) La baja incidencia de contagios en Oruro, indudablemente, se debe a una cuarentena estricta (si no me equivoco, la primera en el país), que merece nuestro reconocimiento porque por el momento no han aumentado los ocho casos iniciales, que de los cuales, según tengo entendido, varios fueron importados por viajeros al exterior (ndR: solo la “paciente cero” es caso importado en Oruro).
Pero debo añadir que también está jugando un rol importante la radiación ultravioleta, nuestro aliado en las ciudades de altura. Eso no significa, sin embargo, que no puedan aparecen otros casos eventualmente, porque existen muchas variables, pero al final de esta pandemia las estadísticas muy probablemente demostrarán que en los lugares de altura hubo menor incidencia.
Esto no significa, sin embargo, que se debe bajar la guardia. También existen otros aspectos técnicos de adaptación a la altura que mencionaremos en una futura oportunidad.
6) El 30 de enero de 2020, en una entrevista de Radio-Tv Universitaria, gracias a una gentil invitación de Johnny Villarroel, quien dirige el programa Desarmado Discursivo, en el que también participó Gonzalo Taboada, presidente de la Academia de Ciencias de Bolivia, afirmé lo siguiente:
Que se deben instalar centros de tratamiento del coronavirus, con salas de terapia intensiva, en áreas alejadas y aisladas de las ciudades para no contaminar. Recomendé que no se lleven a los pacientes a los hospitales centralmente localizados, para dejarlos éstos libres para la atención de las enfermedades habituales.
En el caso de La Paz, sugerí que sea en el altiplano, justamente porque allí existe mayor radiación ultravioleta. Pero además hice una recomendación: posteriormente, las salas de tratamiento de terapia intensiva deberían tener el techo parcialmente de vidrio, como unas claraboyas, para permitir el ingreso de la luz ultravioleta, con el fin de producir la esterilización del ambiente en una forma natural.
Ojalá en el futuro se comprenda la importancia de estas sugerencias.
7) La siguiente gráfica muestra la evolución de las infecciones del coronavirus en Bolivia en la que se observa claramente que en las ciudades de altura (con líneas entrecortadas) hay menor incidencia en función del tiempo:
8) También se recomienda que cuando alguien llegue a su casa y se saque la ropa que usó en la calle, debe exponerla al sol durante esta etapa. Esto permitirá que el virus sea eliminado rápidamente.
9) Es importante mencionar que, como habitantes de la altura, si se llegara a sufrir un caso muy severo que al final evolucionara favorablemente, gracias a los tratamientos de los heroicos médicos, enfermeras y personal de salud en las zonas de altura, las secuelas de las lesiones pulmonares podrían dejar fibrosis (cicatrices), dificultando la capacidad para el ejercicio.
Estas personas desarrollarían en el lapso de más de un mes y medio una poliglobulia (PoliEritroCitemia), que es un mecanismo de compensación frente a la insuficiencia respiratoria crónica.
Es probable que varios puedan permanecer y desarrollar su vida normalmente en la altura con un cuidado médico adecuado.
Finalmente, debo añadir que no se debe bajar la guardia, porque aunque son menos los casos en la altura, existen casos y debemos respetar todos la cuarentena.
Otras recomendaciones pueden ser encontradas en línea en nuestra página web: http://altitudeclinic.com/blog
Gustavo Zubieta-Calleja
Es médico, profesor y director del Instituto Pulmonar y Patología en la Altura (IPPA)
On June 3, 2020, above please note that the incidence in Santa Cruz (2.7 million inhabitants) at 400m above sea level IN GREEN is much higher [12.0 times more] than in the cities of La Paz and El Alto (2.7 million inhabitants) at 3,100m to 4,100mIN DASHED BLUE.
Also, in Beni at 150m IN LIGHT BLUE with only 420,000 inhabitants, (6 times less than in La Paz), already has 3.3 times more cases of COVID-19.
The first graph above is the updated Bolivia SARS-CoVid-2 situation, with the high-altitude low incidence focus. It is linked to our paper
Christian Arias-Reyes1, Natalia Zubieta-DeUrioste2, Liliana Poma-Machicao1, Fernanda Aliaga-Raudan1, Favio Carvajal-Rodriguez1, Mathias Dutschman4, Edith M. Schneider-Gasser3, Gustavo Zubieta-Calleja*2, Jorge Soliz*1,2
1- Institut Universitaire de Cardiologie et de Pneumologie de Québec (IUCPQ), Faculty of Medicine, Université Laval, Québec, QC, Canada. 2- High Altitude Pulmonary and Pathology Institute IPPA. La Paz, Bolivia. 3- Institute of Veterinary Physiology, Vetsuisse-Faculty University of Zurich Winterthurerstrasse 260.
4- Florey Institute of Neuroscience and Mental Health, Gate 11 Royal Parade, 3052, University of Melbourne Victoria, Australia
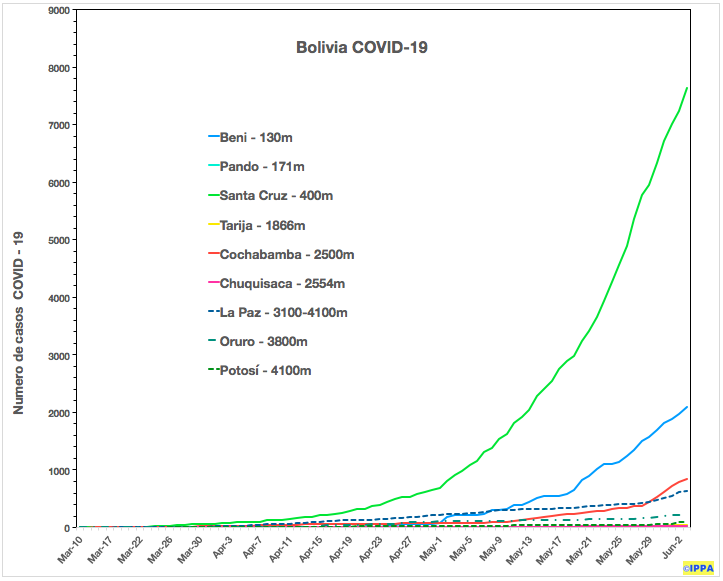
It is an original idea by Prof. Dr. Gustavo Zubieta-Calleja so that COBID-19 information be up-to-date for all readers of our article until the Pandemia stops. Consequently, this scientific article does not become out-dated. Below, is the incidence difference between the lowland cities in Bolivia and that above 3,000m (dashed lines).
The figure below was developed by Favio Carvajal-Rodríguez.
Bolivia incidence as of April 6th, 2020.
Please read the original newspaper article by Prof. Dr. Gustavo Zubieta-Calleja where he is the first in the world to propose that the Coronovirus will have a lower incidence at high altitude:
Extended Longevity at High Altitude published in Dec 2017 at BLDE J where Prof. Dr. Gustavo Zubieta-Calleja expressed for the first time that at high altitude Ultra-Violet radiation serves as an environmental disinfection. These original concepts gave birth to the concept that Coronavirus can have a lower incidence at high altitude.
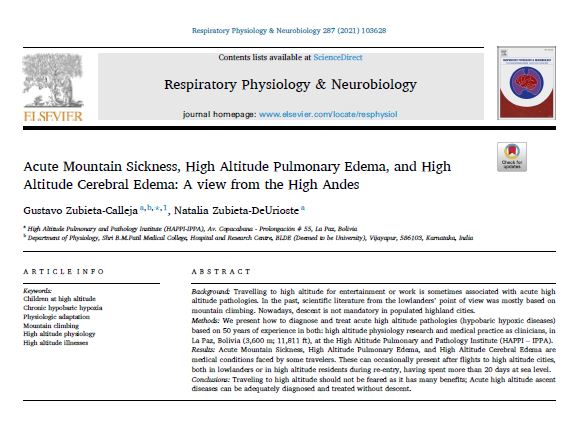

 The original article was printed in the Volume 287, May 2021 of the Respiratory Physiology and Neurobiology journal
The original article was printed in the Volume 287, May 2021 of the Respiratory Physiology and Neurobiology journal