Invited by the Dr. Shyama Narang Foundation President Vasanth Rao for the 2nd International Conference on ALS/MND organized jointly by NIMHANS & Dr. Shyama Narang Foundation 21st-22nd June 2023. Prof. Dr. Gustavo Zubieta-Calleja Head of the High Altitude Pulmonary and Pathology Institute (HAPPI-IPPA) presented his innovative talk “Can Exposure to Hypoxia and Chronic Hypoxia be beneficial in ALS/MND?”.
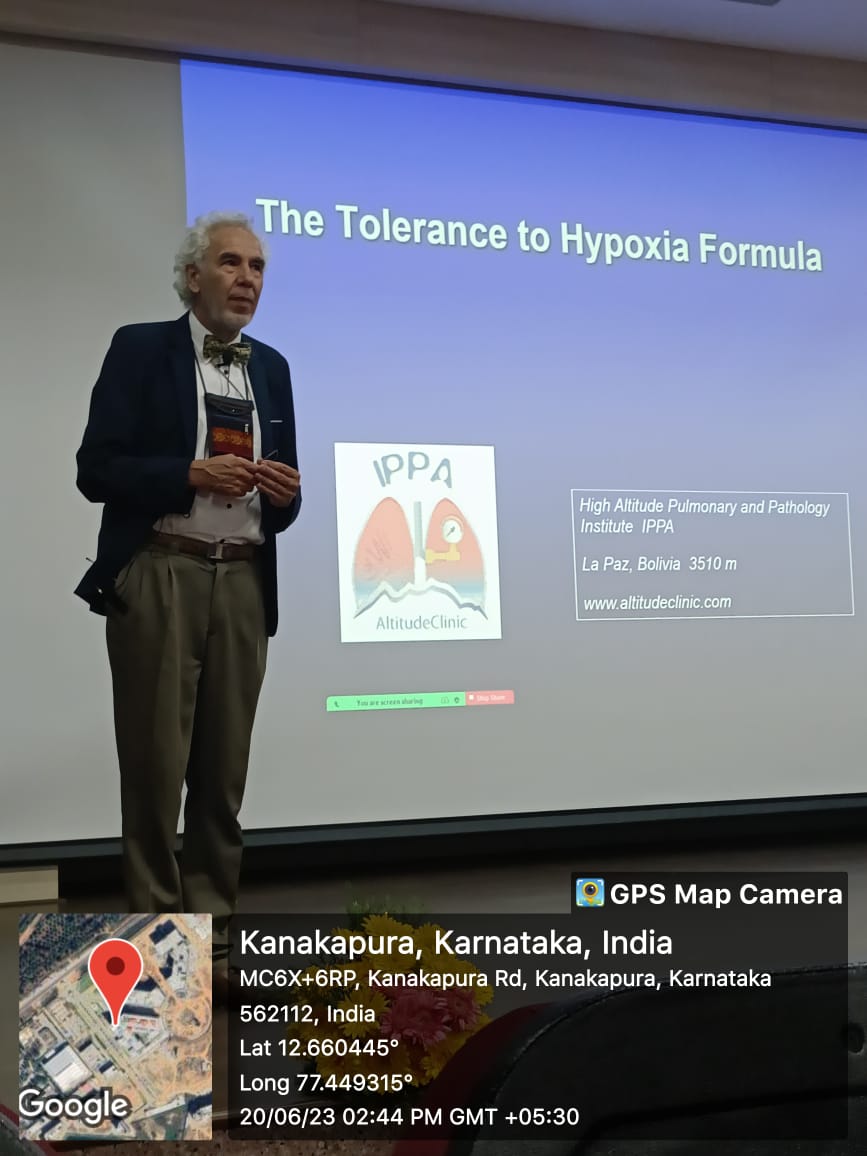
Following the invitation by Prof. Thuppil Venkatesh “The Lead Man of India”, he likewise presented conferences regarding acid-base at high altitude, tolerance to hypoxia, and adaptation to high altitude at different Universities and Hospitals in several cities in the Karnataka area.
Additionally, he participated in the inauguration of the Center for rainforest restoration headed by Dr. Malali Gowda. Finally, he visited outstanding research centers and many temples with magnificent structures. These were nine days of intense activity, travel by plane, train, and car, enjoying the excellent food in different restaurants, and above all re-encounter with very dear friends.
Recognition at the CDSIMER Dr. Chandramma Dayananda Sagar University Institute of Medical Education and Research. Dr. Madan Aekward, Prof. Dr. Gustavo Zubieta-Calleja, Dr. A C Ashok, Prof. Thuppil Venkatesh.With Dr. Madan Aekward, special Officer and Dr. A C Ashok, Principal and Dean of CDSIMER of the Dayananda Sagar University.Dr. Chandramma Dayananda Sagar University Institute of Medical Education and Research.
Group Photo
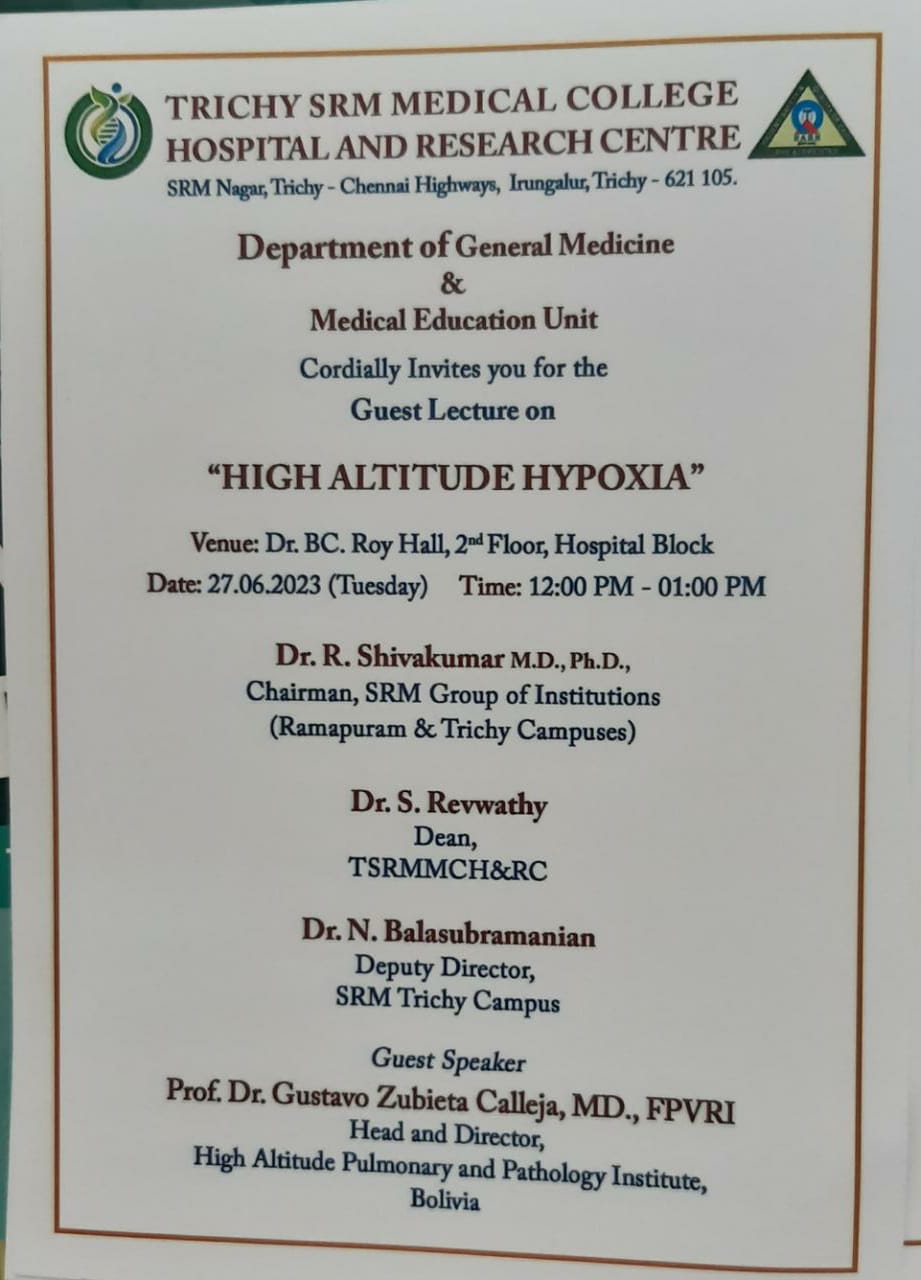
Mr. Vasanth Rao, President of the Dr. Shyama Narang Trust, Prof. Dr. Gustavo Zubieta-Calleja, Prof. Thuppil Venkatesh, Dr. Girdhar Gyani, Dr. Shrivaram K.R. and Dr. Malali Gowda.The speakers of the 2nd International Conference on ALS/MND.With Dr. Pruthvi ChakravarthiCelebrating some beautiful moments at the hostel at NIMHANS. Dr. Girdhar Gyani, Dr. Shirvaram K.R. Prof. Dr. Gustavo Zubieta-Calleja, Prof. Thuppil Venkatesh, Dr. Mahdan Srinivasan and Dr. Malali Gowda.Recognition by Dr. S. Revwathy, Dean of Trichy SRM Medical College Hospital and Research Center.Visiting temples with distinguished colleagues Dr. Parthiban, Dr. T.A. Varkey, Dr. Thuppil Venkatesh.At the Foundation for Quality India in Bangalore. With Prof. Shashi and Prof. Venkatesh, the head of this center. A meeting in Prof. Thuppil Venkatesh’s office at Foundation for Quality India. From Left: Dr. Rhagu, Dr. Gustavo Zubieta-Calleja, Dr. Shivaram K.R. Dr. Thuppil Venkatesh, Dr. Natalia Zubieta (in the screen from Calgary, Canada), Dr. ________, Dr. Malali Gowda, Dr. Madhan Srinivasan.Visiting C-CAMP in Bangalore, one of the most advanced research innovation centers in India.Visiting the advanced laboratories at C-CAMP.Dr. Malali Gowda, The Gene Man of India, Prof. Dr. Gustavo Zubieta-Calleja, The Hypoxia and Oxygen Man of the World and Prof. Thuppil Venkatesh, The Lead Man of India.
Atending a wedding ceremony by invitation of Prof. Thuppil Venkatesh.Dr. Abbas Ali, Vice-Chancellor of ERA University in Lucknow, India Dr. Girdhar Gyani , Director General at ASSOCIATION of HEALTHCARE PROVIDERS in Dehli, India, Prof. Dr. Gustavo Zubieta-Calleja for the High Altitude Pulmonary and Pathology Institute (HAPPI-IPPA) in La Paz, Bolivia.
Receiving a blessing by an elephant.
Inauguration of the Center for Rainforest Restoration by Dr. Malali Gowda in Anuganaly, Hassan Karnataka, India.The tree Prof. Dr. Gustavo Zubieta-Calleja planted at the Center for Rainforest Restoration.Planting a bush in the rocks for the project Center for Rainforest Restoration.Guyani, Gustavo Zubieta, Thuppil Venkatesh and Malali Gowda.Observing the biodiversity with Dr. Shivaram K.R. Prof. Thuppil Venkatesh, Prof. Dr. Gustavo Zubieta-Calleja and Dr. Malali Gowda (first and last from DNAi World. Sharing a wonderful dinner with Dr. Parthiban, Dr. T.A. Varkey, Dr. Thuppil Venkatesh.A wonderful re-encounter with Dr. Girdhar Gyani from Quality India in Dehli and Dr. Krishna, cardiovascular surgeon in Bangalore. He came to Bolivia to one of the Chronic Hypoxia Symposiums.Dr. Parthiban, Dr. Thuppil Venkatesh and Prof. Dr. Gustavo Zubieta-Calleja at Magapallupuram templeAt Magapallupuram temple. Dr. Parthiban, Master E. Shakthi Saran (Dr. Elangovan’s son), Dr. Thuppil, Dr. Zubieta-Calleja At Magapallupuram temple. Dr. Parthiban, Dr. Thuppil, Dr. Zubieta-Calleja and Dr. S. Elangovan.At Magapallupuram temple. Dr. Parthiban, Dr. Zubieta-Calleja, Dr. Thuppil, and Dr. S. Elangovan.
At Magapallupuram temple. Dr. Zubieta-Calleja, Dr. Parthiban, Dr. S. Elangovan and Dr. Thuppil Venkatesh.
[12:09, 12/5/2022] Gustavo Zubieta: Dear Dr. Meera: [12:10, 12/5/2022] Gustavo Zubieta: Wonderful article! Very detailed and extensive. Congratulations, well done!!! Thank you for citing me!! All the best!! [12:12, 12/5/2022] +91 86100 66441: 🙏💐it was a pleasure to have met the scientific community through the conference. Your thoughts and work mean a lot to ayurveda. It will establish ayurveda’s scientificity in the long run.. A few centuries from now.. [12:13, 12/5/2022] +91 86100 66441: You are much ahead.. Our world is much behind Dr Gustavo [12:19, 12/5/2022] Gustavo Zubieta: I am truly impressed on how you have interpreted our work. Splendid because you understand the concepts!!! Ayurveda has great wisdom instilled, and it results from millenary experience and the adequate use of intelligence based on doing good for the well-being of the whole world community. It also uses nature to heal. That is magnificent!!! Thank you so much for those sincere and warm words, which honor us greatly!! Hope to meet you soon in the near future!!
Once again, we had a magnificent scientific and friendly event on Oct 10-14, 2022. We had outstanding speakers from around the globe and a great scientific program. We thank all of you for helping us make this a great event in chronic hypoxia unique in the world.
We thank all the organizers that did a splendid job! The full details can be found here.
During the conference at CIBA at Titicaca Lake.
At the auditorium in front of the Titicaca Lake 8CHS.With the commanders of the High Altitude Diving Instruction Center (CIBA).The CIBA Hyperbaric Chamber
International Undergraduate Medical Students´ Research Conference of INFORMER
Bench to Bedside: Translational Medicine. Era University ConferenceBench to Bedside: Translational MedicineBench to Bedside: Translational Medicine
Professor Hari Sharma and Professor Doctor Gustavo Zubieta-CallejaBench to Bedside: Translational Medicine Prof. Thuppil VenkateshBench to Bedside: Translational Medicine
Professor Lindsay BrownBench to Bedside: Translational Medicine
Doctor Roli MathurBench to Bedside: Translational Medicine
Professor Abbas Ali Mahdi
Winner of the first prize of the Science and Technology Plurinational prize by the Ministry of Education, Bolivia 2021 as the leader of a group of researchers under the theme “Effect of life at high altitude on incidence and severity of COVID-19
This unique logo shows what he is. The Mountain (Thorax diaphragms) is Illimani (6,432m), caressing the city of La Paz, Bolivia (3,100-4,100m). The lung at high altitude, above the mountain shown with a barometer with low levels of oxygen: Hypoxia…… (art by Katia Ardaya-Zubieta).
PROF. DR. GUSTAVO ZUBIETA-CALLEJA, M.D., FPVRI The HYPOXIA MAN (India 2017) Head High Altitude Pulmonary and Pathology Institute (HAPPI-IPPA) located in La Paz, Bolivia (3,100-4,100m) in the heart of South America. Cel (591-73258026) gzubietajr@altitudeclinic.com Av. Copacabana – Prolongación # 55 Teleféricos Celeste y Blanco Av. Del Poeta, La Paz, Bolivia
Carries out joint research with his daughter Dr. Natalia Zubieta-DeUrioste, MD. They collaborate with BLDE University India, Laval University, Canada.
BUT, WHO IS HE REALLY?
……. Well… kind of difficult to say. He has been described as a “Renaissance Man” along with his father Prof. Dr. Gustavo Zubieta-Castillo, because of his extensive know-how.
He constructed with his father Prof. Dr. Gustavo Zubieta-Calleja the Chacaltaya Glass Pyramid Laboratory at 5,260masl, the highest laboratory in the world.
He has been invited to give talks in many parts of the world, including: India (5 times) USA Italy Ukraine Russia Spain Germany Poland Denmark Czech Republic Ecuador Colombia Brazil Chile Japan Tibet China
And many more…
Interested in learning more about him? Go to his blog. Make sure you navigate all around.
He constructed pulmonary function equipment, protein electrophoresis equipment, and even an elevator.
He is a top self-taught mechanical electronics engineer.
He developed hardware, software for medical records and on-line data loggers since 1981, being the first to have databases in the medical field.
Distinctions and Awards: Several, but he is not interested. Rather, he created the “Science, Honor and Truth” Award
His publications are extensively read:
Publications by Prof. Dr. Gustavo Zubieta-Calleja ordered by date.
[1] Zubieta-Castillo G, Zubieta-Calleja R, Zubieta-Calleja G. Estudios sobre la circulacion coronaria en la altura. Acta de las Primeras Jornandas de Medicina y Cirugia de la Altura; 1978 4 – 7 de Octubre La Oroya, Peru; 1978. [2] Zubieta-Castillo G, Zubieta-Calleja, G. & Zubieta-Calleja, R. El consumo de oxigeno en miocardio de perros a 3600 mt y a differentes tensiones de oxigeno. Acta de las primeras Jornadas de Medicina y Cirugia de la altura. La Oroya, Peru 1978. [3] Zubieta-Calleja G, Zubieta-Castillo, G., Zubieta-Calleja, R. La Produccion de anhidrido carbonico durante el consumo de oxigeno en miocardio de perros a 3600 m. (Abstracto). Primer Congreso Boliviano de Biología; 1979 1979; UMSS Cochabamba; 1979. [4] Zubieta-Castillo G, Zubieta-Calleja, R., Zubieta-Calleja, G. Clasificacion de la eritrocitosis en la altura de acuerdo al numero de eritrocitos (Abstracto). Primer Congreso Boliviano de Biología; 1979; UMSS Cochabamba; 1979. [5] Zubieta-Castillo G, Zubieta-Calleja GR. Chronic mountain sickness and miners (Spanish). Revista de la Academia Nacional de Ciencias de Bolivia. 1985;4:109-16. [6] Zubieta-Castillo G, Zubieta-Calleja GR. El mal de Montaña Cronico y los mineros. (Chronic mountain sickness and miners). Cuadernos Academia Nacional de Ciencias de Bolivia. 1985;62:109-16. [7] Zubieta-Castillo G, Zubieta-Calleja GR. Pulmonary diseases and chronic mountain sickness (Spanish). Revista de la Academia Nacional de Ciencias de Bolivia. 1986;5:47-54. [8] Zubieta-Castillo G, Zubieta-Calleja GR. Las Enfermedades pulmonares y el Mal de Montaña Cronico. (Pulmonary diseases and chronic mountain sickness). Cuadernos de la Academia Nacional de Ciencias de Bolivia. 1986;68:3-12. [9] Zubieta-Castillo G, Zubieta-Calleja GR. The triple hypoxia syndrome at altitude (Abstract). Amer Rev of Respir Dis. 1988;137(4):509. [10] Zubieta-Castillo G, Zubieta-Calleja GR. Iatrogenic Disease in a polycythemic patient at altitude. Amer Rev of Respir Dis. 1988;137(4):509. [11] Zubieta-Calleja GR, Zubieta-Castillo G. High Altitude Pathology at 12000 ft. La Paz: Publisher: Papiro, 1989. La Paz, Bolivia [12] Zubieta-Castillo G, Zubieta-Calleja GR. Progressive high altitude hypoventilation reversed by hyperoxia. Amer Rev of Respir Dis. 1990;141(4):a924. [13] Zubieta-Castillo. G & Zubieta-Calleja G. Hematocrit, PaO2 and PaCO2 changes in a High altitude increased Polycythemic during a 12 year follow up. Amer Rev of Respir Dis. 1990;141(4):a921. [14] Zubieta-Castillo G, Zubieta-Calleja, G & Zubieta-Calleja, L. Cambios en la PaO2, PaCO2 y el hematocrito en un paciente con mal de montaña cronico durante 12 años. Acta del Quinto Congreso Nacional de Medicina de la Altura; 1992; La Oroya, Peru; 1992. p. 136. [15] Zubieta-Castillo G, Zubieta-Calleja G. Acute Hypoventilation on ascent to high altitude. European Respiratory Society Congress; 1992; Vienna, Austria; 1992. [16] Zubieta-Castillo G, Zubieta-Calleja GR. El Sindrome de Triple Hipoxia en la Altura. Acta del Quinto Congreso Nacional de Medicina de la Altura; 1992; La Oroya, Peru; 1992. p. 136. [17] Zubieta-Castillo G, Zubieta-Calleja G. Eritrocitosis agudas, EPOC y sindrome de triple hipoxia. Acta del Quinto Congreso Nacional de Medicina de la Altura; 1992; La Oroya, Peru; 1992. p. 135. [18] Zubieta-Calleja G, Zubieta-Castillo G. High altitude illness in Bolivia (Abstract). First World Congress of High Altitude Medicine and Physiology; 1994; La Paz, Bolivia: Edvil;p. 58.
[20] Zubieta-Calleja GRZ-C, G and Zubieta-Calleja, L. Zubieta-Calleja, G.R. Zubieta-Castillo, G and Zubieta-Calleja, L.. Inadequate treatment of excessive erythrocytosis. Acta Andina. 1995;4:123-6. [21] Zubieta-Calleja GZ-C, G. Chronic Mountain Scikness. Proceedings of the Third Symposium on High Altitude Medicine and Physiology; 1995; Xining, Gingai, PR China; 1995. p. 40. [22] Triplett J, Zubieta-Calleja L, Zubieta-Castillo G, Zubieta-Calleja GR. Physiological changes related to rapid altitude shifts in La Paz, Bolivia. Acta Andina. 1996;5(1):19-21. [23] Zubieta-Calleja GR, Zubieta-Castillo G. High Altitude Pathology Institute. 1996 [cited 2007 june 15, 2007]; Available from: http://www.altitudeclinic.com [24] Zubieta-Calleja G. and Zubieta-Castillo GR. International Soccer vetoed in Stadiums above 3000 m of altitude. International Society for Mountain Medicine. 1996;6(1). [25] Zubieta-Calleja GR, Zubieta-Castillo, G and Zubieta-Calleja, L. Can HAPE be diagnosed through the tongue? Acta Andina. 1996;5:31-4. [26] Zubieta-Castillo G, Zubieta-Calleja G. Triple hypoxia syndrome. Acta Andina. 1996;5(1):15-8. [27] Zubieta-Castillo G, Zubieta-Calleja G. New Concepts on chronic mountain sickness. Acta Andina. 1996;5:3-8. [28] Zubieta-Calleja G, De Urioste, L. & Zubieta-Calleja, L. High altitude residents in Bolivia. Progress in Mountain Medicine and High Altitude Physiology. In: HidekiOhno TK, Shigeru Masuyama and Michiro, Nakashima, ed. Progress in Mountain Medicine and High Altitude Physiology. Matsumoto, Japan 1998:185-9. [29] Zubieta-Calleja G, Zubieta-Castillo G. Changes in oximetry during breath holding in normal residents of high altitude. In: Hideki Ohno TK, Shigeru Masuyama and Michiro, ed. Progress in Mountain Medicine and High Altitude Physiology. Matsumoto, Japan 1998:343-8. [30] Zubieta-Castillo G, Zubieta-Calleja G, Arano E, Zubieta-Calleja L. Respiratory Disease, chronic mountain sickness and gender differences at high altitude. In: HidekiOhno TK, Shigeru Masuyama and Michiro, Nakashima., ed. Progress in Mountain Medicine and High Altitude Physiology. HidekiOhno, Toshio Kobayashi, Shigeru Masuyama and Michiro, Nakashima. 1998:132-7. [31] Zubieta-Castillo G, Zubieta-Calleja GR. Pulse oximetry in chronic mountain sickness- long breath holding time and oscillation at lowest saturation. In: HidekiOhno TK, Shigeru Masuyama and Michiro, Nakashima, ed. Progress in Mountain Medicine and High Altitude Physiology 1998:349-54. [32] Pollard AJ, Niermeyer S, Barry P, Bartsch P, Berghold F, Bishop RA, et al. Children at high altitude: an international consensus statement by an ad hoc committee of the International Society for Mountain Medicine, March 12, 2001. High Alt Med Biol. 2001 Fall;2(3):389-403. [33] Zubieta-Calleja G, Zubieta-Castillo, G., Zubieta-Calleja, L. & Zubieta, N. Exercise performance of bolivian aymara in 3 conditions: at La Paz 3,510 m, breathing a hypoxic mixture simulating Chacaltaya and at Chacaltaya 5,200 m. HAMB. 2002;3(1):114-5. [34] Zubieta-Calleja G, Zubieta-Castillo, G., Zubieta-Calleja, L., Zubieta, N. Measurement of circulatory time using pulse oximetry during breath holding in chronic hypoxia. HAMB. 2002;3(1):115. [35] Zubieta-Calleja GR, Zubieta-Castillo, G., Zubieta-Calleja, L., Zubieta, N. Breath holding and pulse oximetry as a diagnostic tool at high altitude. HAMB. 2002;3(1):115. [36] Zubieta-Calleja GR, Zubieta-Castillo, G., Zubieta-Calleja, L., Zubieta, N. Exercise performance in chronic mountain sickness (cms) patients at 3510 m. HAMB. 2002;3(1):114-5. [37] Zubieta-Castillo G, Zubieta-Calleja, G.R., Zubieta-Calleja, L. Exercise performance in a woman with CMS following triple hypoxia syndrome treatment. HAMB. 2002;3(1):114-5. [38] Zubieta-Castillo G, Zubieta-Calleja, G.R., Zubieta-Calleja, L., Zubieta, N. Bolivian Aymara that played soccer at 6542 m maintain higher oxygen saturation and lower oxygen uptake during maximal exercise. HAMB. 2002;3(1):114-5. [39] Zubieta-Castillo G, Zubieta-Calleja GR, Zubieta-Calleja L, Zubieta C, Nancy. Adaptation to life at the altitude of the summit of Everest. Fiziol Zh. 2003;49(3):110-7. [40] Zubieta-Calleja (Jr) GR, Moretti M, Zubieta-Calleja L, Zubieta N, Zubieta-Castillo (Sr) G. Chronic mountain sickness among the Chipaya after 2500 years of high altitude exposure. HAMB. 2004;5(2):291-2. [41] Zubieta-Calleja (Jr) GR, Zubieta-Castillo (Sr) G, Zubieta-Calleja L, Zubieta N. Hypoventilation in Chronic Mountain Sickness: a mechanism to preserve energy. HAMB. 2004;5(2):291-2. [42] Zubieta-Calleja G. Bloodletting: a medical resource since the stone age. Journal of Qinghai Medical College. 2004;25(4):273-5. [43] Zubieta-Castillo (Sr) G, Zubieta-Calleja (Jr) GR, Zubieta-Calleja L, Zubieta N. How chronic mountain sickness (cms) contributed to the theory of life at the hypoxic levels of the summit of Mount Everest. HAMB. 2004;5(2):291-2. [44] Fabiola León-Velarde, Marco Maggiorini, John T Reeves, Almaz Aldashev, Ingrid Asmus, Luciano Bernardi, Ri-Li Ge, Peter Hackett, Toshio Kobayashi, Lorna G Moore, Dante Penaloza, Jean-Paul Richalet, Robert Roach, Tianyi Wu, Enrique Vargas, Gustavo Zubieta-Castillo, Gustavo Zubieta-Calleja. Consensus statement on chronic and subacute high altitude diseases. High Alt Med Biol. 2005 Summer;6(2):147-57. [45] Paulev PE, Zubieta-Calleja GR. Essentials in the diagnosis of acid-base disorders and their high altitude application. J Physiol Pharmacol. 2005 Sep;56 Suppl 4:155-70. [46] Zubieta-Calleja GR, Zubieta-Castillo G, Paulev PE, Zubieta-Calleja L. Non-invasive measurement of circulation time using pulse oximetry during breath holding in chronic hypoxia. J Physiol Pharmacol. 2005 Sep;56 Suppl 4:251-6. [47] Zubieta-Calleja GR, Paulev PE, Zubieta-Calleja L, Zubieta-Calleja N, Zubieta-Castillo G. Hypoventilation in chronic mountain sickness: a mechanism to preserve energy. J Physiol Pharmacol. 2006 Sep;57 Suppl 4:425-30. [48] Zubieta-Calleja GR, Zubieta-Castillo G, Zubieta-Calleja L, Zubieta N. The increase in hematocrit during the high altitude adaptation process. (Abstract). Wilderness Environ Med. 2006 Fall;17(3):202-3. [49] Zubieta-Castillo G, Sr., Zubieta-Calleja GR, Jr., Zubieta-Calleja L. Chronic mountain sickness: the reaction of physical disorders to chronic hypoxia. J Physiol Pharmacol. 2006 Sep;57 Suppl 4(2):431-42. [50] Paulev P-E, Zubieta-Calleja G. High Altitude Diving Depths. Res in Sports Med. 2007;15(1 or 2 in print). [51] Zubieta-Calleja GR, Paulev P-E, Zubieta-Calleja L, Zubieta-Castillo G. Altitude adaptation through hematocrit changes. J of Physiol and Pharmacol. 2007;58(Supplement). [52] Zubieta-Castillo G, Zubieta-Calleja GR. Facts that Prove that Adaptation to Life atExtreme Altitude (8848m) is Possible. In: L.Lukyanova NTaPKS, editor. Adaptation Biology and Medicine: Health Potentials; 2007; New Dehli, India: Narossa Publishing House; 2007. [53] Gustavo Zubieta-Calleja GZC, Poul-Erik Paulev (2009) The Adaptation of Highlanders to Sea Level. In Wilderness & Environmental Medicine- Wilderness Conference and Annual Meeting. (ed.), Vol. 20, pp. 184-5, Wilderness & Environmental Medicine-Official Publication of the Wilderness Medical Society, Snowmass, Colorado. [54] Zubieta-Calleja G, Zubieta-Castillo G, Zubieta-Calleja L, Ardaya-Zubieta G, and Paulev PE (2009) Do over 200 million healthy altitude residents really suffer from chronic Acid-Base disorders? Indian J Clin Biochem 26, 62-5. [55] Zubieta-Calleja L (2009) The High Altitude Adaptation Formula. In 36th Annual Conference of Association of Clinical Biochemists of India. (ed.), Vol. 24, pp. 83-4, Indian Journal of Clinical Biochemistry- Association of Clinical Biochemists of India, Kochi, India. [56] Zubieta-Castillo G (2012) Loss of Adaptation and Maladaptation: two terms Inadequately used-Conversely-“Adaptation: A Fundamental Law of Biology that at High Altitude, even Permits Life at the Hypoxic Levels of Mt. Everest”. In Global Hypoxia Summit & 4th International Conference on Chr onic Hypoxia. (ed.), Vol. pp. 74-5, New Delhi, India. [57] Zubieta-Calleja, G, Zubieta-Castillo, G, Merishi, J. (2012) Extremely high altitude hypoxic conditions during Mount Everest expeditions, residence at South Pole stations, in Tibet and among the Andes: Van Slyke equation modification is crucially important for acid–base measurements. Journal of Biological Physics and Biochemistry 12(3):103-112. [58] Balaban DY, Duffin J, Preiss D, Mardimae A, Vesely A, Slessarev M, ZubietaCalleja G, et al.(2013) The in-vivo oxyhaemoglobin dissociation curve at sea level and high altitude. Respir Physiol Neurobiol 186, 45-52. [59] Zubieta-Calleja, GR, Ardaya, G, Zubieta-DeUrioste, N, Paulev, PE, Zubieta-Castillo, G. Tolerance to Hypoxia (2013) Vol 59:4 Fiziol Journal. Kiev, Ukraine. [60] Zubieta-Castillo, G and Zubieta-Calleja GR.(2014) High Altitude Research and its Clinical Application. Chapter in Book Translational Research in Environmental and Occupational Stress. Editors: Chachi Bala Singh, Nanduri R. Prabhakar, Crinivas N. Pentyala. Springer India. [61] Zubieta-Calleja GR, Zubieta-DeUrioste NA. Extended longevity at high altitude: Benefits of exposure to chronic hypoxia. BLDE Univ J Health Sci 2017;2:80-90 [62] Zubieta-Calleja, G.R.; Zubieta-DeUrioste, N.; Venkatesh, T.; Das, K.; Soliz, J. COVID19: Multiple Diseases Simulating Extreme High-Altitude Exposure? Oxygen Transport Physiology and Scarce Need of Ventilators; Andean Condor’s-Eye-View. Preprints 2020, 2020050085 (doi: 10.20944/preprints202005.0085.v1). [63] Zubieta-Calleja, G., & Zubieta-DeUrioste, N. (2020, September 27). Pneumolysis and “silent hypoxemia” in COVID-19. https://doi.org/10.31219/osf.io/qde8w [64] Roberto Carlos Vera, Natalia Zubieta-DeUrioste, Gustavo Zubieta-Calleja, (Oct 2020) La quema de los bosques bolivianos afecta la calidad del aire y atenta contra la salud en estos tiempos de pandemia COVID- https://zuniv.net/pub/BOLET%C3%8DN1Ambiente_13oct.pdf. [65] Arias-Reyes C, Zubieta-DeUrioste N, Poma-Machicao L, Aliaga-Raduan F, CarvajalRodriguez F, Dutschmann M, Schneider-Gasser EM, Zubieta-Calleja G, Soliz J. Does the pathogenesis of SARS-CoV-2 virus decrease at high-altitude? Respir Physiol Neurobiol. 2020 Jun;277:103443. doi: 10.1016/j.resp.2020.103443. Epub 2020 Apr 22. PMID: 32333993; PMCID: PMC7175867. [66] Soliz J, Schneider-Gasser EM, Arias-Reyes C, Aliaga-Raduan F, Poma-Machicao L, Zubieta-Calleja G, Furuya WI, Trevizan-Baú P, Dhingra RR, Dutschmann M. Coping with hypoxemia: Could erythropoietin (EPO) be an adjuvant treatment of COVID-19? Respir Physiol Neurobiol. 2020 Aug;279:103476. doi: 10.1016/j.resp.2020.103476. Epub 2020 Jun 6. PMID: 32522574; PMCID: PMC7275159. [67] Gustavo R. Zubieta-Calleja*, Natalia Zubieta-DeUrioste, Thuppil Venkatesh, Kusal K. Das and Jorge Soliz, “COVID-19 and Pneumolysis Simulating Extreme High-altitude Exposure with Altered Oxygen Transport Physiology; Multiple Diseases, and Scarce Need of Ventilators: Andean Condor’s-eye-view”, Reviews on Recent Clinical Trials (2020) 15:
https://doi.org/10.2174/1574887115666200925141108 [68] Zubieta-Calleja, G., Merino-Luna, A., Zubieta-DeUrioste, N., Armijo-Subieta, NF., Soliz, J., Arias-Reyes, C. , Escalante-Kanashiro, R., Carmona-Suazo, J., López-Bascope, A., Calle-Aracena, J., Epstein, M. & Maravi, E (2020, October 15). COVID-19 patients in the high-altitude areas of Bolivia and Peru manifest a substantive decrease in mortality. https://doi.org/10.31219/osf.io/7rd2h [69] Zubieta-Calleja G, Zubieta-DeUrioste N. Pneumolysis and “Silent Hypoxemia” in COVID-19. Indian J Clin Biochem. 2020 Nov 9;36(1):1-5. doi: 10.1007/s12291-020-00935-0. Epub ahead of print. PMID: 33191989; PMCID: PMC7652053. [70] Zubieta-Calleja G, Merino-Luna A, Zubieta-DeUrioste N, Armijo-Subieta NF, Soliz J, Arias-Reyes C, Escalante-Kanashiro R, Carmona-Suazo JA, López-Bascope A, Calle-Aracena JM, Epstein M, Maravi E. Re: “Mortality Attributed to COVID-19 in High-Altitude Populations” by Woolcott and Bergman. High Alt Med Biol. 2021 Feb 9. doi: 10.1089/ham.2020.0195. Epub ahead of print. PMID: 33567217. [71] Zubieta-Calleja G, Zubieta-DeUrioste N. Acute Mountain Sickness, High Altitude Pulmonary Edema, and High Altitude Cerebral Edema: A view from the High Andes. Respir Physiol Neurobiol. 2021 Feb 2;287:103628. doi: 10.1016/j.resp.2021.103628. Epub ahead of print. PMID: 33545376. [72] Zubieta-Calleja G, Zubieta-DeUrioste N. The Oxygen Transport Triad in High-Altitude Pulmonary Edema: A Perspective from the High Andes. International Journal of Environmental Research and Public Health. 2021; 18(14):7619. https://doi.org/10.3390/ijerph18147619