
http://zuniv.net/symposium7
Hello from our beautiful La Paz, Bolivia 4100 to 3100m, one of the 7 marvel cities of the world.
And it continues to grow:
Always remembering our Mountain Guru Gustavo Zubieta-Castillo (Sr.).
and thanking him for his extraordinary academic legacy !!
His genes are now in a third generation, Natalia Zubieta De-Urioste who is now our brand new M.D.
and a transcendental member of our team at the High Altitude Pulmonary and Pathology Institute.
Gustavo Sr. must indeed be proud !
_______________________________________________________________
The concept about hypoxia is always negative. The problem is that it is a biased opinion. There is a constant search for the deleterious effects of hypoxia. However, several adaptation mechanisms are misinterpreted as being a negative response, when they are actually an extraordinary positive effect.
We have to remark once more: Humans live longer at high altitude !!! Please read our latest publication:
This paper is the most popular paper on the BLDE Journal in that issue:
Furthermore, It has had such a high impact, that we have even been invited to write a book on the subject.
We are changing the concept of Chronic Hypoxia, around the globe. Understand why we are invited to give talks in many outstanding places:
 She was born on Oct 28, 1900 in San Pedro de Buena Vista Potosi, Bolivia at 3850m of altitude. According to the US Gerontology Research group – that documents the oldest people on the planet- the bolivian Julia Flores would be the oldest woman alive since she is 6 months older than the japonesa Chiyo Miyako, born on May 2 1901. Please read the article on Newspaper Pagina 7 here. At the opening session in the ABCICON ______________________________________________
Come join us to discuss these and other Chronic Hypoxia interesting aspects.
After 6 successful Chronic Hypoxia Symposiums (5 held in Bolivia and 1 in India) we invite you to join us and participate in the forthcoming, exciting:
7th Chronic Hypoxia Symposium
February 23- March 2, 2019
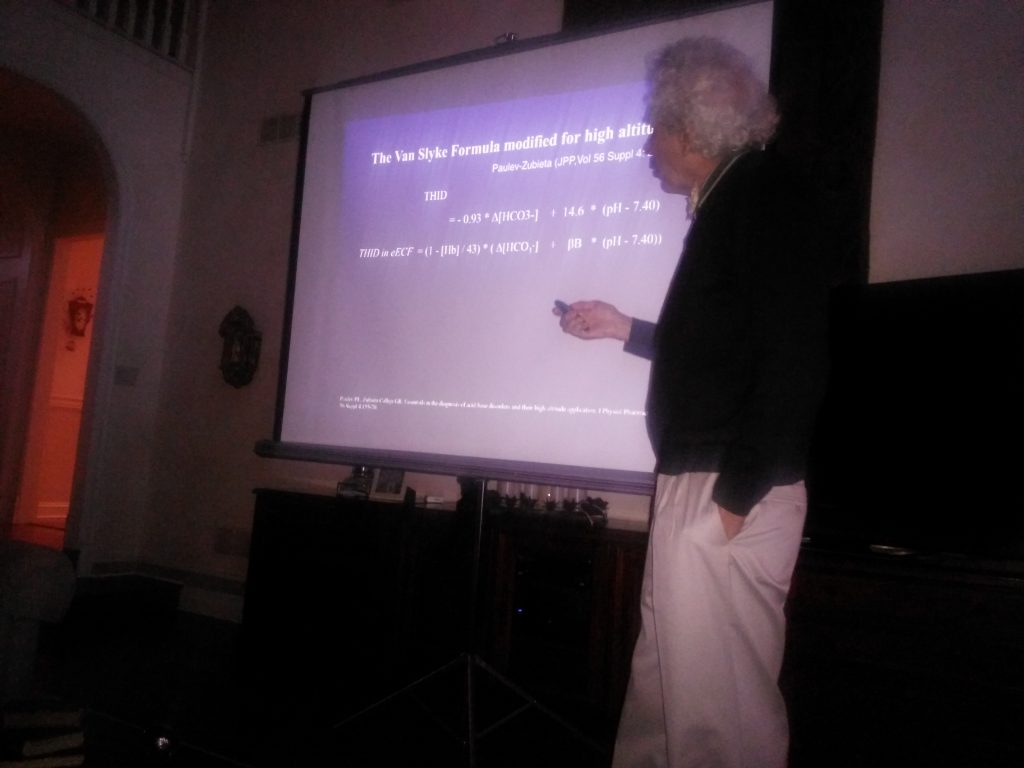
Dedicated to the late extraordinary Danish Physiologist Poul-Erik Paulev Poul-Erik Paulev, Ole Siggard-Andersen and Gustavo Zubieta-Calleja at the University of Copenhagen 2005Mark your calendar! This year we will also attend the Carnaval in Oruro 3800m. We want to show you how people dance with great energy over several kilometers and some carrying heavy 20 kilogram outfits. No one worries about hypoxia. As affirmed in our publications: The best way to defeat hypoxia is a timely exposure to chronic hypoxia __________________________________________________________________
Other news
Conferences in USA, 2018
This time we were in the wonderful USA, to give talks about our scientific experience in chronic hypoxia. It was a splendid and unique experience.
We started with a talk at the National Institutes of Health in Washington. Another in Pennsylvania for the local Geriatrics Society. The next at the Center for Space and Planetary and Sciences in the University of Arkansas.
The last talk was at Tulane Medical School in New Orleans, Louisiana.
Read about it here:
http://www.altitudeclinic.com/usa-2018
______________________________________________________________
Space flight under Chronic Hypoxia. One more step in Human BioSpaceFormin.
Get a sneak pre-print preview of this paper at ResearchGate.
|
Category Archives: Meetings


Grand USA Chronic Hypoxia Tour 2018
Between April 18th and April 30th Prof. Dr. Gustavo Zubieta-Calleja, Director and Head of the High Altitude Pulmonary and Pathology Institute in La Paz, Bolivia, gave talks explaining the benefits of Life under Chronic Hypoxia (low-oxygen).
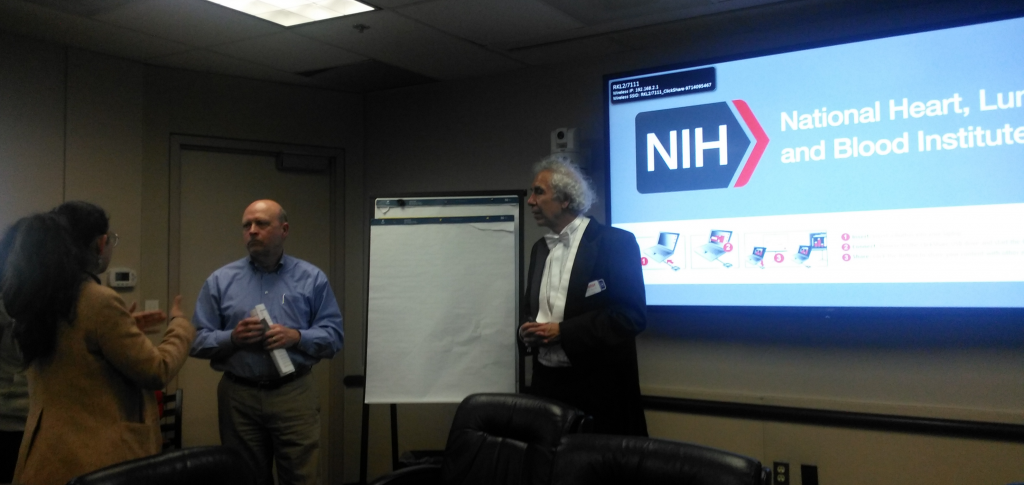
It started with a talk on April 18th at the National Institutes of Health, National Heart Heart, Lung and Blood Institute in Bethesda Maryland, in the Division of Lung Diseases. It’s director Dr. James Kyley introduced Prof. Zubieta to a group of his top Staff scientists.

The presentation was entitled: “Benefits of exposure to Chronic Hypoxia: Adaptation, Tolerance to Hypoxia, Acid-Base at high altitude and future space travel”. It was a stimulating talk that has a different concept regarding the traditional fears of hypoxia in Sea level physicians. This talk showed that chronic hypoxia at high altitude residents gives rise to many advantages, as a way of adaptation.
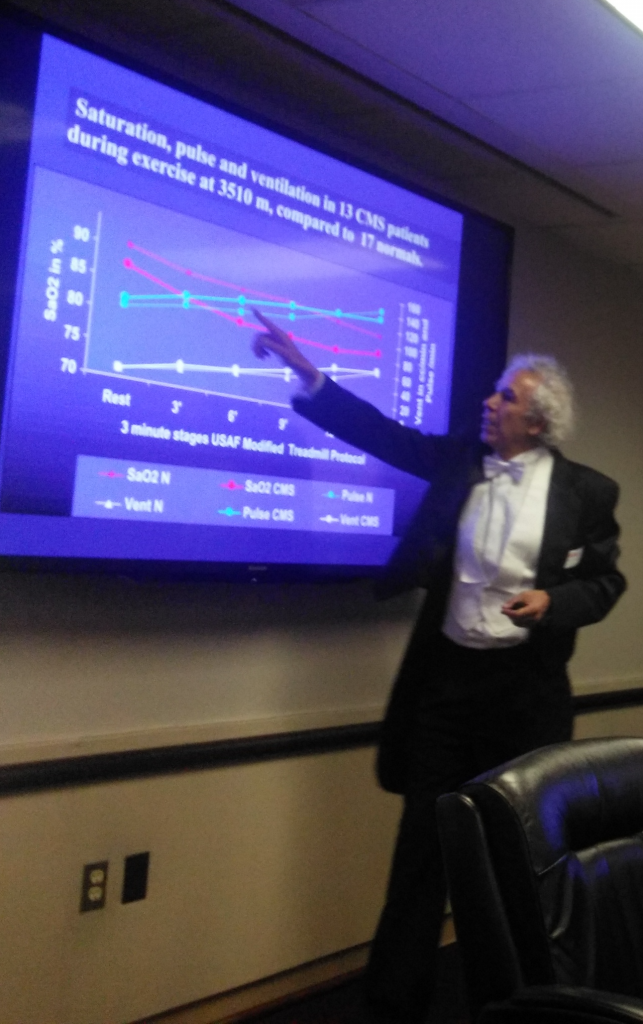
Explaining exercise at high altitude

Among them he showed that Bolivians live longer at high altitude in the high altitude areas.
http://www.bldeujournalhs.in/article.asp?issn=2468-838X;year=2017;volume=2;issue=2;spage=80;epage=90;aulast=Zubieta-Calleja
This scientific paper is the most popular article in that journal thus far, since its publication on Dec 15, 2017. We have also been invited to write a book on this subject. So this is a transcendental paper in high altitude medicine.

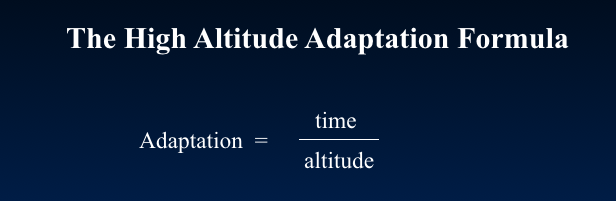
However many other subjects were dealt with in the conference, like the Adaptation Formula that we developed.
And the Remarkable Tolerance to Hypoxia formula that we also created:
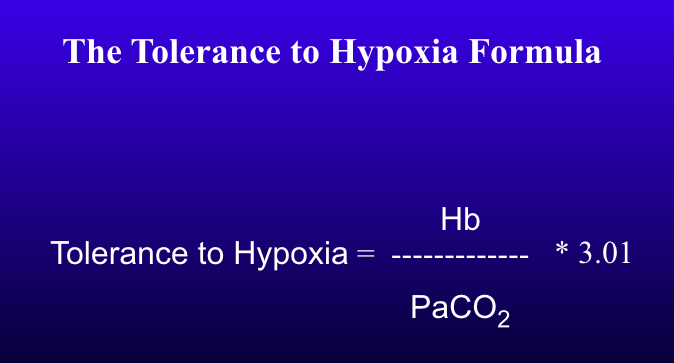
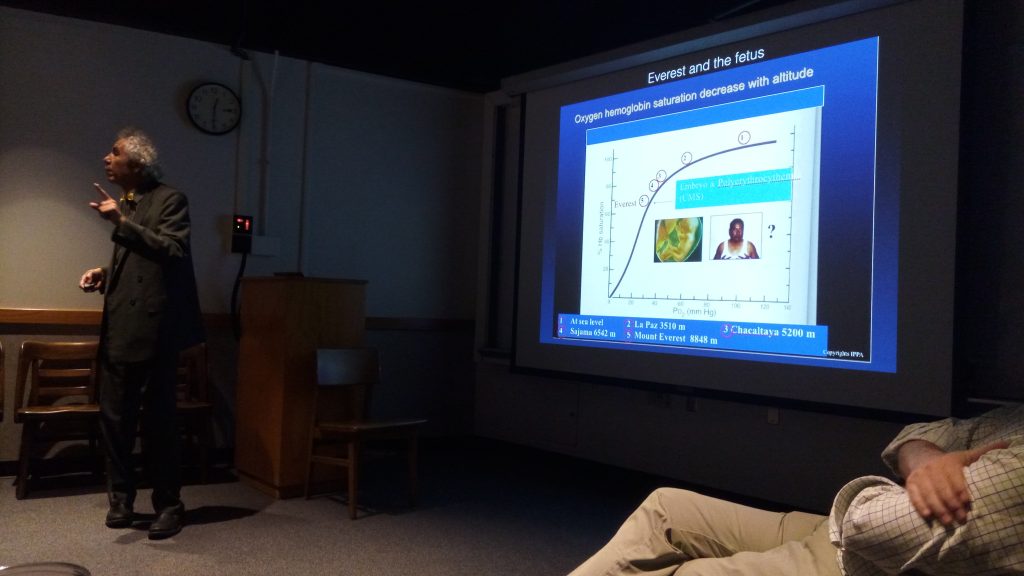
This formula shows that paradoxically, the higher man goes to high altitude the more tolerance to hypoxia there is. Compared to sea level, the high altitude residents of La Paz, are 1.7 times more tolerant to hypoxia. Similarly, on the summit of Mt. Everest, where humans have climbed to, without the assistance of oxygen, it is around 6 times. This outstanding capacity of survival in such low levels of oxygen is proof that nature has wisely granted living beings the mechanisms to survive and sustain life even in the extreme environments.


We then moved on to meet Dr. Oscar Murillo, a distinguished Geriatrician in Pennsylvania.

He kindly hosted a conference dinner at his beautiful residence in Schneksville, Penssylvania. The dinner was great. The members of the Geriatrics Society were a delight to share moments with.

Among them, Dr. Steven Fuller, a most distinguished Geriatrician with whom we shared many interesting comments regarding high altitude physiology.



Our next stop was Fayetteville, Ark where Prof. Zubieta-Calleja gave a talk at the Center for Space and Planetary Sciences in the University of Arkansas.

He had attended this University during a year as a Pre-med before his transfer to the Universidad Mayor de San Andres Medical School in La Paz, Bolivia. Prof. Dr. Gustavo Zubieta-Calleja, was an exchange student in Little Rock, Arkansas and lived with the Smith Family in 1973 prior to attending to the University of Arkansas.

Mr. Jim Youngblood, working for NASA, had met and acquainted astronaut Ed White of the Apollo program, who had given, as a Christmas present, an autographed photo to his son Tom Youngblood, currently a Pediatrician married to Cindy Smith. Astronaut Ed White was one of the three astronauts that unfortunately died in the tragic prelaunch burn of Apollo 1. Such event initiated the sea level (760mmHg), in space cabin pressure flights with 21% oxygen.
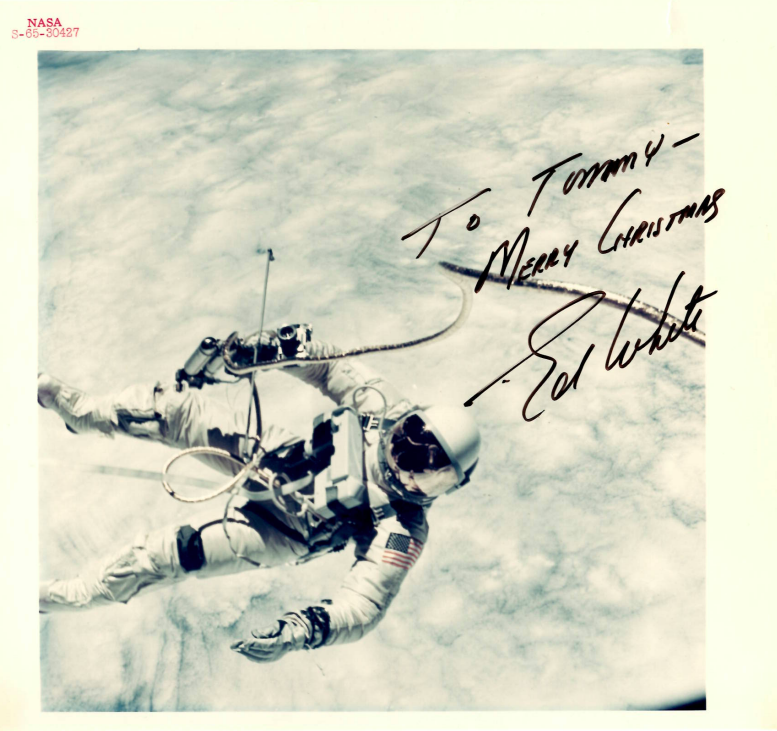
This coincidence of meeting Mr. Jim Youngblood in the dinner prior to the talk on space travel, is truly extraordinary, since for Prof Dr. Gustavo Zubieta-Calleja’s talk proposes that high altitude pressures (495mmHg) similar to the city of La Paz (3600m) be used in space capsules instead.
The title of the talk for the Center for Space and Planetary Sciences was about “Space travel under Chronic Hypoxia“.


It was in relation to an original idea of Prof. Zubieta-Calleja back in 2007 as expressed in his book “Adaptation to High Altitude and to Sea Level: Acid-Base Equilibrium, Ventilation and Circulation in Chronic Hypoxia“.

The idea is that future space travel has to be undertaken in high altitude environment similar to the city of La Paz (3600m), within space capsules.

This would grant astronauts great advantages. It would allow for a practical solution to astronauts anemia in Space. Furthermore, it would give great advantages speeding up the possibility of going out of the space ship and using a space suit, since the pressure changes would not be as great. This would allow for much lighter space suits, aiding in the flexibility and maneuverability.

Much more will come from this revolutionary concept, that will change forever the way humans travel in space. Please click below to see the BLDE Journal pre-print:
https://www.researchgate.net/publication/325536733_Space_travel_in_a_high_altitude_environment_One_more_step_in_human_BioSpaceFormin
All these ideas are born from over 48 years of experience in our Institute, founded by the late Prof. Dr. Gustavo Zubieta-Castillo:
The final talk was given at Tulane Medical School in New Orleans, Louisiana.

This was a very special situation. On a previous conference talks organized by Prof. Thuppil Venkatesh in Dec 2017 throughout India, Prof. Zubieta-Calleja, had the opportunity to meet Prof. Dewan S.A. Mahid at Prof Kusal Das’ Laboratory in BLDE University in Vijayapur, India. Prof. Majid a most distinguished scientist of the Physiology Department at Tulane, invited Prof Zubieta-Calleja to go give a talk.
Prof. Zubieta-Calleja had been in New Orleans when he was 8 years old during two years because Prof. Dr. Gustavo Zubieta-Castillo was a visiting Professor at Tulane Medical School back in 1964.
We had a special bonus as we met our dear friend Prof. Rafael Rubio and Cherry his wife for the second time in beautiful New Orleans.

We had the most interesting discussions about science and likewise, Rafael and following the extraordinary coincidences, Rafael had worked with Gustavo Zubieta-Castillo (Sr) in the 60’s at the Instituto de Cardiologia in Mexico. They had published a joint paper entitled “RUBIO, R., and-ZUBIETA, G.: ‘The variation of the electrical resistance of microelectrodes during the flow of current’, Acta Physiologica Latin Americana, 1961, 11. “, which became a very cited reference in physiology.

Top row from left: Prof. Zubieta-Calleja, Prof. Edwan Mahid, Daniel from Bangladesh. Prof. Rafael Rubio, Seated from left: Cherry Rubio, Rafaela Zubieta, Dr. Natalia Zubieta DeUrioste, NIna Mahid, Mrs. Daniel
Dr. Rafael Rubio obtained his PhD in US and became a Professor of physiology at University of Virginia during over 30 years, becoming Emeritus. He now resides permanently in New Orleans and had written his book “Endothelial Luminal Membrane-Glycocalyx: Functionalities in Health and Disease” at Tulane.


The talk was carried out on April 30, 2018 at the Physiology Department which runs under the direction of Prof. Gabriel Navar. It was a pleasure to meet him and to discuss subjects of mutual interest.
He heads the Center for Biomedical Research Excellence in Hypertension and Renal Biology and has a staff that is truly outstanding. The program of visits is below:
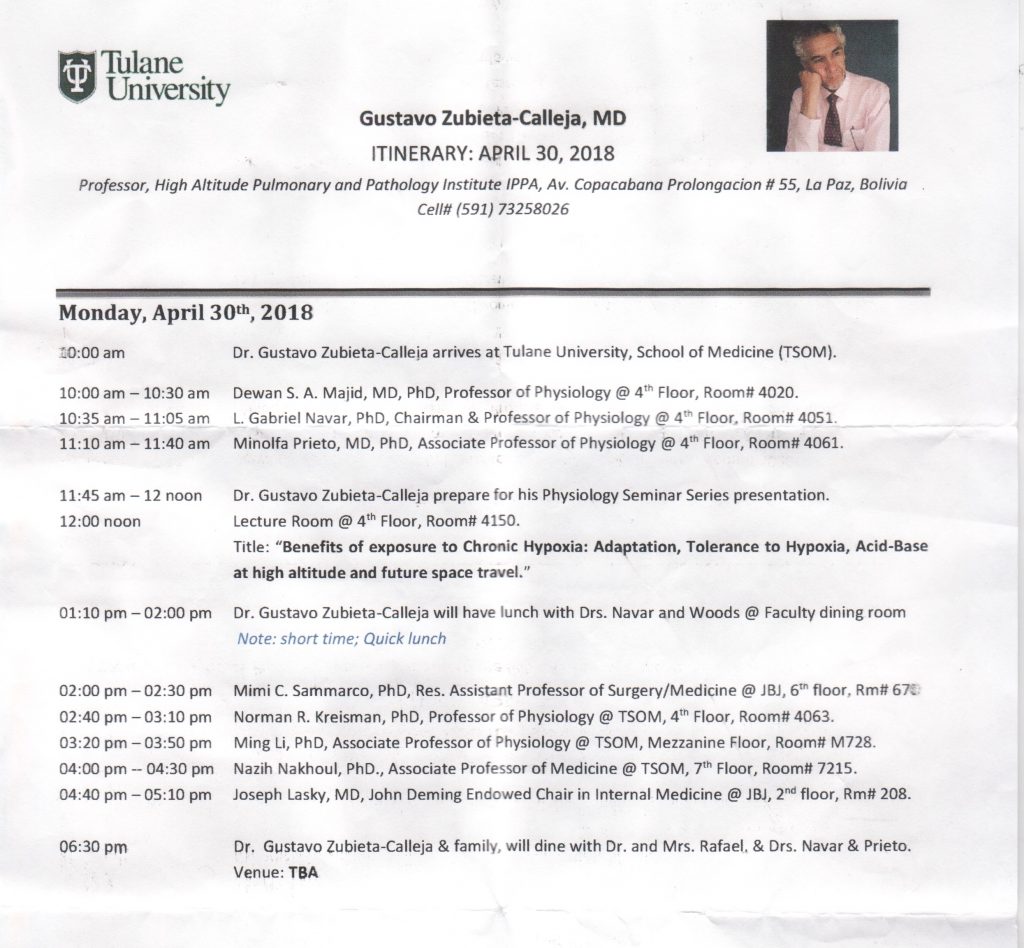
We truly enjoyed meeting such distinguished colleagues at Tulane, and particularly Dr. Minolfa Prieto.
In this opportunity Prof. Dr. Gustavo Zubieta-Calleja was with his IPPA team, his brand new colleague and scientific researcher Dr. Natalia Zubieta, our language expert Rafaela Zubieta and Lucrecia De Urioste our International Relations expert.

Come join us at the 7th CHRONIC HYPOXIA SYMPOSIUM in Feb 2019 !!

India conferences 2017
India 2017 Conferences
Nov 29 – Dec 15, 2017
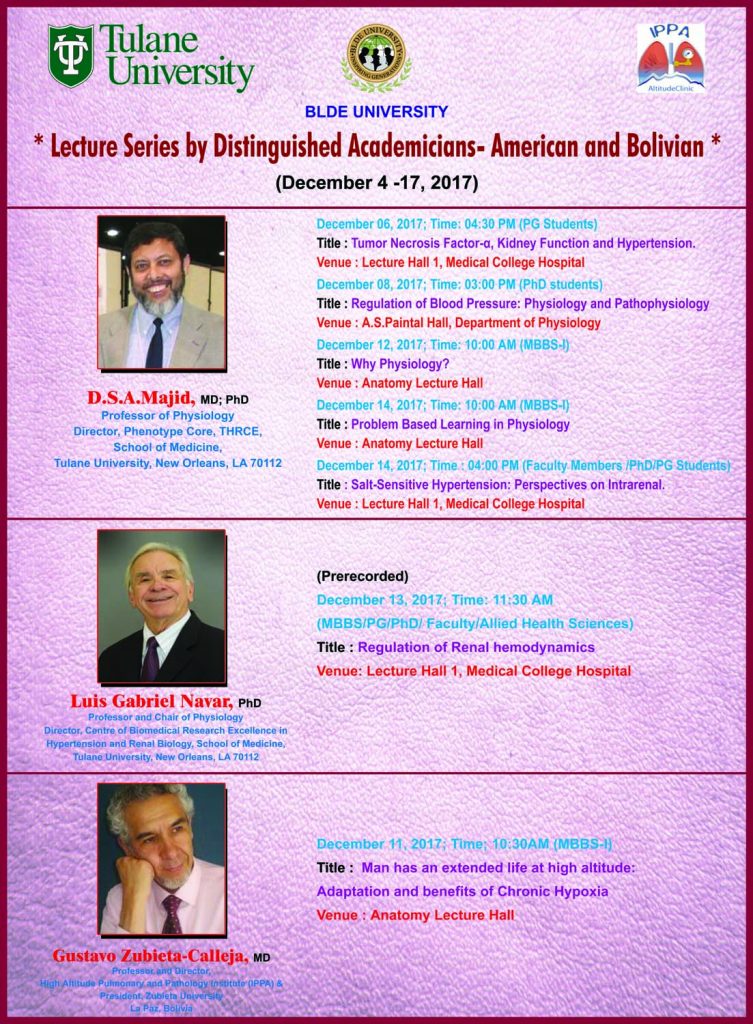
Once again Prof. Dr. Gustavo Zubieta-Calleja was invited to participate in ACBICON (Association of Clinical Biochemists of India Conference, and to give talks at BLDE University between Nov 29 and Dec 15, 2017. Prof. Thuppil Venkatesh, was the host and he organized several conferences and meetings along with some visits to temples and friends in Bangalore, Lucknow, and Vijayapur. Here is his description of the events.
The inauguration was carried out by Prof. M.L.B. Bhatt, Vice-Chancellor of the famous KING GEORGE’S UNIVERSITY in Lucknow. His speech was very interesting and full of oratory talent. He talked about “The Lead Man” referring to the famous Prof. Thuppil Venkatesh and added that also present was “The Hypoxia Man” referring to me. I felt touched by such kind denomination. Many colleagues then started calling me “The Hypoxia Man” the rest of the meeting, which obviously makes it easier for them than to say my name that is complicated in India, as you may appreciate. They often confuse my First name Gustavo with my Last name Zubieta-Calleja. These are handicaps of cultural differences.





Prof. Abbas Ali Mahdi, the previous Head of the Biochemistry Department at King George’s University and now Vice- Chancellor of Era University, was the organizer of this interesting meeting in Lucknow. There I had the opportunity of meeting once again Prof. Praveen Sharma, the Head of the Biochemistry of the All India Institute of Medical Sciences in Jodhpur and Chief Editor of the Indian Journal of Biochemistry. I was invited to participate in the editorial board of the Journal and had the privilege of attending the yearly meeting.
My conference was entitled:
Clinical Biochemistry at the summit of Mt. Everest: Correct interpretation of arterial blood gases and acid-base status.
We then flew back to Bangalore where we met some old friends like Parthasarathy and Shashi.
We then travelled by train to Vijayapur and where we spent 4 days in multiple activities at the distinguished BLDE University Physiology Department that is more than 100 years old. We were greeted once more, by Prof. Kusal Das Head of the Laboratory of Vascular Physiology and Medicine
With Professor of Physiology Dewan Majid of Tulane Medical School, we shared very pleasant moments along with Prof. Thuppil Venkatesh and Parthasarathy.
I gave a talk related to chronic hypoxia and how high altitude residents have achieved what we call an “advantage for survival” and where I explained that we observe that sea level residents have a very poor tolerance to hypoxia, inducing us to affirm that they suffer a “disability”, whereby they have poor response to hypoxia and in contrast high altitude residents can even achieve extended longevity.
Incidentally, a researcher wrote:
If any one else knows any high altitude cities in the world where there is extended longevity please let us know by sending us an email: zubieta@altitudeclinic.com

Prof. Thuppil Venkatesh and myself also gave talks at the engineering Department at BLDE, thanks to an invitation by Prof. Swastika Das.

These were two very stimulating talks that generated much enthusiasm in the Professors and students of such a distinguished engineering School.


I was also invited to be the External Examiner for a PhD Thesis by Dr S S Devarmani, Controller of Examination, BLDE University in reference to:
After an interesting presentation and round of questions by the assisting Professors of BLDE, and then followed by a closed meeting with further questions and recommendations, between the Three examiners: Prof. Kusal Das, Prof. Gustavo Zubieta-Calleja and Prof. Manjunath Aithal the guiding professor, along with the student Praveen S. Patil, we decided to accept and approve the Thesis and I was granted the honor of announcing it to the candidate.
There were several other activities but upon returning to Bangalore, I was invited by Satish Jain, President of the Maharaja Agrasen Hospital, to inaugurate the new Fertility Unit. Please see the video.
Aside from our Scientific cooperation with BLDE University with Prof. Kusal Das, we are now proud to announce that Dr. Abbas Ali Mahdi has honored me as:
Visiting Professor at Era University Lucknow, India
Visiting Professor at American University in Barbados
Thereby we establish a promising future collaboration association.
Our most profound thankfulness to Prof. Venkatesh and all his colleagues for the wonderful visit.

6th Chronic Hypoxia Symposium Follow-up
Chronic Hypoxia Symposium VI – Follow-up
Oct 10 – 16, 2016
La Paz, Bolivia
Dedicated to the late Prof. Dr. Gustavo Zubieta-Castillo
This unique itinerant symposium was a gathering of participants from around the world, all sharing a common interest in the wonder of the mountain environments, whether through research or other endeavors. With Chairman Dr. Gustavo Zubieta-Calleja at the helm, assisted by his family, medical students and Dr. Fabian Wayar. This symposium convened in La Paz (3100 – 4100m), and was generously supported by the High Altitude Pulmonary and Pathology Institute (IPPA) with collaboration by the Bolivian Navy, the La Paz Medical College and its President, Dr. Luis Larrea and the Universidad Franz Tamayo “Unifranz.” All were engaged in the lively presentations, and were wholly encouraged to participate in topic discussions.
Details of the Conference
The conference presentations were given almost exclusively in English. Attendees met in the Unifranz on the first day on Monday Oct 10, 2016, where opening words were given by Prof. Dr. Gustavo Zubieta-Calleja, Director of the High Altitude Pulmonary and Pathology Institute (IPPA) and Dr. Thuppil Venkatesh, President of the International Society of Chronic Hypoxia. This symposium was poignantly dedicated in the memory of the incomparable Dr. Gustavo Zubieta-Castillo, whose life was devoted to the study of hypoxia and the care of patients suffering from altitude illness. A presentation by Dr. Zubieta-Castillo’s granddaughter, Natalia Zubieta, highlighted his life’s work. Conference participants were provided with books commemorating Dr. Zubieta-Castillo with quotes from colleagues who respected and admired him and his work from around the globe.

Dr. Giuseppe Miserocchi, former Professor of Physiology and Biophysics at the University Milano-Bicocca in Italy, gave an enlightening talk on the Inter-individual Differences in the Adaptive Response of the Lung to Hypoxia. Dr. Miserocchi described the conditions leading to lung edema, including miscrovascular permeability and increased cardiac output, versus the conditions opposing it, including interstitial matrix rigidity, vasoconstriction in pulmonary microcirculation, and reduced capillary patency. Variations exist among human response to diffusion capacity of the lungs during hypoxia, with more than half of the subjects showing an increase in alveolar membrane diffusing capacity that overpowered the decrease in lung capillary blood volume.
Dr. Zubieta-Calleja gave a lively presentation regarding The Road to “Defeating Hypoxia” is a timely exposure to chronic hypoxia. He also discussed polyerythrocythemia as a precise terminology developed by the late Prof. Dr. Gustavo Zubieta-Castillo, to be used instead of chronic mountain sickness. He reiterated the simple yet powerful formula:
Adaptation = time / altitude
Dr. Zubieta-Calleja challenged the belief that people life’s under chronic hypoxia is debilitating, arguing that many conditions may be treated with exposure to hypoxia. He gave evidence of increased longevity among high-altitude dwellers. He punctuated his talk by climbing on a chair and “punching” hypoxia, breaking it into pieces that fell down in the screen, to emphasize its defeat!

After several breaks, in which the conference attendees enjoyed tasty local cuisine such as salteñas, cunapes, and galletas, Dr. Benedito Honorio Machado from the School of Medicine of Riberao Preto in the University of Sao Paolo, Brazil presented “Neural Mechanisms Involved in Autonomic and Respiratory Changes in Rats Submitted to Short-Term Sustained Hypoxia.” In this talk, Dr. Machado described the role of short-term sustained hypoxia on anesthetized rats in increasing the sympatho-inhibitory and bradycardiac components of baroreflex, as well as the sympathetic and respiratory responses of peripheral chemoreflex. They found hypoxic exposure was associated with increased excitation of the nucleus tractus solitarius neurons on the carotid body and aortic depressor nerve. Changes in glial density were also noted.
Dr. Alla Portnychenko, Head of the International Centre for Astronomical, Medical and Ecological Research, NAS of Ukraine presented via webcam “Rebuilding of carbohydrate and lipid metabolism under hypoxia: Regularities and therapeutic possibilities.” Her studies on rats showed activation of hypoxia inducible factor 1a (HIF-1a) and -3 a subunits during hypoxia, resulting in the induction of GLUT-4 and -1 in the myocardium and lungs. This resulted in a change from carbohydrate to predominantly lipid substrate up-regulation. In humans, they found changes in cholesterol metabolism, leptin and insulin-growth factor IGF-1 plasma levels, and positive correlation with HIF-dependent protein IFG-1 and HDL-cholesterol. She concluded with the intriguing suggestion that hypoxia might be used to correct metabolic disorders in some people.
Dr. Zoya Serebroska of the Bogomoletz Institute of Physiology in Ukraine presented via webcam “Potential application of cerium dioxide nanoparticles for acute pneumonia treatment.” She and her team found that CeO2 nanoparticles significantly reduced morphological and functional pulmonary damage in rats after exposure to pneumonia. It was noted that Dr. Serebroska’s mother Dr. Tatiana Serebrovskaya, also a hypoxia researcher, was one of the first to suggest the role of nitric oxide as an important molecule in vasodilatory regulation.
Dr. Walter Calderon of the Hospital Nacional Ramiro Prialé, EsSalud, Huancayo, Junín, Perú and the Universidad Nacional del Centro del Perú, Huancayo, Perú presented “Prospective Validation of Framingham Criteria for Congestive Heart Failure diagnosis in a High Altitude Population” He noted that sensitivity was 98.6% for patients with Heart Failure, but specificity of these criteria were only 12% among patients who presented with dyspnea and at least one of the major Framingham criteria. He showed a compelling picture of collateral circulation from a cardiac cath.
Dr. Jose Antonio Carmona Suazo of the Hospital Juarez in Mexico presented “CO2 reactivity, a tool for prevention of HACE (High Altitude Cerebral Edema): Hands-on workshop.” He gave an exciting hands-on demonstration of the non-invasive and safe ability to monitor the level of cerebral blood flow, ETCO2 in humans at altitude. Cerebral and respiratory effects were measured on Dr. Thuppil Venkatesh, who happily volunteered.
The Tiwanaku Código 0.4666 was presented by Willy Eduardo Cortez Hemzler, Investigador y Artista Plástico. Señor Cortez described how he discovered that the ratio of the length and width of the building materials at Tiwanaku equals 0.46, which is maintained throughout the structures. He showed the relationship of 0.46 to the radius of a circle.
After this, participants were treated to a bus tour of the city of La Paz.and the Inauguration Ceremony was held at the IPPA Building auditorium.
It was a lively ceremony, with honored by the presence of 4 ambassadors (Great Britain, Mexico, European Union and Italy) and the representative of the Consulate of India, along with the representatives of the La Paz Medical College, Unifranz and the Bolivia. The La Paz Mayor’s office through its representative, granted Prof. Thuppil Venkatesh the “Huesped Ilustre de la ciudad de La Paz” (Distinguished Guest of the city of La Paz), normally given only to outstanding personalities (like Presidents) that visit our city.


On Tuesday, October 11, participants left early in the morning to the ruins Tiwanaku and the Archaeological Museum, at 3800m. The morning provided a fascinating tour of the grounds of unknown age. Willy Eduardo Cortez Hemzler was the impromptu tour guide. The attendees also saw the big Monolito Bennet at Tiwanaku, and visited the ruins of Punta Punku, believed to be even older than Tiawanaku.

After this intriguing look at Bolivian history and life since ancient times at high altitude, participants had a late lunch on the Barco Multiproposito of the Bolivian Army. We were received in true elegance and style by the Army. Talks continued with Dr. Giuseppe Miserocchi continuing his presentation on “Inter-individual differences concerning the oxygen diffusion-transport function in the lung.” One fascinating thing we learned was that middle-distance runners tend to fare poorly at altitude, due to increased permeability at the alveolar level!
Next, presented Rajashekar Nanjappa of the Regional General Manager, THE HINDI NEWSPAPER, Bengaluru, India Media & Mountain Medicine A Commitment: Role and Impact of Media on Society and with Special reference to Newspapers role in Public Awareness. He focused on the endeavors of LESAAT which has organized treks at high-altitude around the globe.
After these presentations, attendees returned to La Paz at Unifranz and viewed the poster competition entries. These were “Development and validation of new sepsis criteria at high altitude” by Dr. Walter Calderon-Gerstein, and “Spirometry values of high-rise residents” of La Paz, Bolivia by one of the medical students, both awarded the 100 US$ price donated by Prof. Thuppil Venkatesh, President of the International Society of Chronic Hypoxia.


On Wednesday, October 12, participants rose early for the bus ride to Lake Titicaca at 3800m. Participants visited the High Altitude Diving Training Center in Tiquina.

Here, talks were given by the Comander of the Diving Center, Cap. Chavez who described in Spanish the history and workings of the Dive Center (CIBA) and the challenges encountered while diving at altitude (buceo en altura). After a delicious lunch tasting the high altitude lake trout, participants toured the hyperbaric chamber and the hospital boat located on the base.

Other talks that day included “Low Altitude Peripheral Edema (LAPE): The opposite of HAPE or HACE” by Prof. Dr. Gustavo Zubieta-Calleja, on the swelling (positive Godet sign) that occurs when high-altitude residents spend time in low-altitude environments. He described the changes in sialic acid levels obtained from red blood cells in his family after a trip to low-altitude destinations in India.

A pre-recorded lecture by Dr. Sadykova from the Institute of Mountain Physiology National Academy of Sciences, Kyrgyz Republic described the neuroendocrine changes occurring at altitude. Among those, elevated norepinephrine, dopamine, serotonin, TSH and T4, and a reduction of testosterone and T3 were noted.

KVR Tagore, President of LESAAT, then described “Mountains – Law – Ethics ,” and discussed the importance of protecting mountains as precious resources through sustainable tourism.
Finally, Willy Eduardo Cortez Hemzler took time to finish his lecture from Monday on Tiwanku and the code of 0.466.
After these presentations, attendees returned to La Paz at Unifranz and viewed the poster competition entries. Two were granted the first prize of 100 US$ donated by Prof. Thuppil Venkatesh, President of the International Society of Chronic Hypoxia. These were: “Development and validation of new sepsis criteria at high altitude” by Dr. Walter Calderon-Gerstein, and “Spirometry values of high-rise residents” of La Paz, Bolivia by one of the medical students.

On Thursday, October 11, participants traveled initially to the Refugio of Huayna Potosi and later to Chacaltaya (5260m). Scores of llamas and alpacas were photographed by the curious attendees, some of whom even got to view a glimpse of the shy and reclusive vicuña!

In Chacaltaya, Nam Deo of Bangalore, India gave a talk “Vihangam Yog helps in high altitude chronic hypoxia” and led the group in meditation on the shoulder of the mountain.

Interestingly, one of the participants reported that her pulse oximetry reading increased from 89% to 93% after the meditation session, Dr. Zubieta-Calleja, explained that as reported in one of his papers, breath holding at high altitude can momentarily increase the SpO2 to even sea level values of 98%.. Dr. Thuppil Venkatesh then gave a speech about “Life in high altitude conditions.” Prof. Sadashivaya, gave an interesting talk about the importance of “forestation at high altitude”. Prof. Nanjapa of the Hindu Newspaper talked about high altitude and the media, K.V.R Tagore talked about philosophical aspects of mountain climbing. Prof. Satish Jain also mentioned about his experience with high altitude.
Finally Prof. Dr. Gustavo Zubieta-Calleja, gave a talk about the evolution of high altitude medicine, the tolerance to hypoxia at high altitude and thanked everyone for participating in this outstanding symposium, where the visit to different altitude sights to show normally developing life is a one of the fundamental objectives of defeating the wrong concepts of hypoxia.
All these talks filmed outdoors with the Chacaltaya Pyramid “the highest laboratory in the world 5250m)” (shown in the background), created by the late Prof. Dr. Gustavo Zubieta-Castillo and his son Prof. Dr. Gustavo Zubieta-Calleja, in conjunction with the Club Andino Boliviano.

Upon returning to La Paz, a dinner and closing ceremony was held at the residence of Prof. Dr. Gustavo Zubieta-Calleja in the southern residential area of Calacoto. It was a special gathering where Dr. Satish Jain assisted in preparing some food from India, along the food that Lucrecia De Urioste with her assistant, Lucia, Natalia and Rafaela so beautifully presented for all those attending. Some talks also took place here.



Dr. Giuseppe Misserochi presented Dr. Zubieta-Calleja with a gift of a water color painting of the Cordillera, that he personally painted while enjoying the beatufil mountains around La Paz.

Nam Deo from India, leaded everyone in a meditation session in the living room.

Awards and certificates were presented and the Symposium was closed.

The colleagues and friends from India, joined us in a trip to visit the incredible Salt Lake, Potosi and Sucre. Life at high altitude flourishes everywhere!

See you in the VII Chronic Hypoxia Symposium in two years!!
written by Annie Wislowski
Edited by Prof. Dr. Gustavo Zubieta-Calleja

Chronic Hypoxia Symposium VI
VI Chronic Hypoxia Symposium
Dedicated to the late Prof. Dr. Gustavo Zubieta-Castillo (Sr.)
October 8-13, 2016
Mark your calendar! Visit our website.
We thank all the colleagues that have expressed their interest to participate.
New concepts about Chronic Hypoxia
We think that Chronic Hypoxia has to be looked upon in a different manner than how it is seen today. For anyone visiting us, you will find an active, busy modern city in the bowl shaped city of La Paz and El Alto. The streets are filled with people, in their daily routine, going up and down the streets, some quite steep. How many are concerned that they are living between 4100m and 3100m? I could almost affirm: NONE. However some foreigners do feel the altitude as they are comparing it with sea level. But many of those start living here and adapt perfectly well. They also end up forgetting they are at high altitude!


The city of La Paz with much construction of buildings going on, lately.
How about sports at high altitude?
Some of you may recall the soccer game we carried out in the summit of Mountain Sajama at 6542m. under the leadership of Gustavo Zubieta-Castillo (Sr.)

Did you know that several bicycle world speed records have been broken in La Paz? The lower density of the air is an advantage. Hypoxia is not a drawback.
and how about the 100m dash?
The current men’s world record is 9.58 seconds, set by Jamaica’s Usain Bolt in 2009, while the women’s world record of 10.49 seconds set by American Florence Griffith-Joyner in 1988 remains unbroken.
We think that the 100 meter dash world record could also be broken here!!! Lets propose it and see if it is true. Falciform anemia, if by any chance present, could of course be a major drawback.

And about disease at high altitude?
We have to quote Dr. Thuppil Venkatesh, President of the Chronic Hypoxia Society: “I always keep thinking how two individuals (you and your Dad) with no resources could bring the world together to have a rethinking about the Physiology at High altitude as a way of life and not as sickness. you both.”.
We are naturally most thankful for his kind words.
We see the increase of red blood cells as a blessing, not a culprit. In fact we are happy when red blood cell counts increase. At high altitude, in our experience, anemia reduces your capacity for exercise, polycythemia does not. The most adequate terminology, as created by the late Gustavo Zubieta-Castillo (Sr). is Polyerythrocythemia.
Poly-erythro-cyt-hemia = Poly (many) + Erythro (red) + cyt (cells) + hemia (blood).
Can Chronic Hypoxia help in space travel and new settlements?
In our previous conferences we have proposed that space capsules have the same barometric pressure as La Paz (1/3 less than at sea level). This would help in energy resources, allow for longer travel, facilitate and speed the change of reducing pressure of the environment for the extravehicular suits to 1/3 of the sea level barometric pressure.


These are some of the advantages of chronic hypoxia.There are many more.
Are we (high altitude dwellers) afraid of life at sea level?
At high altitude, we are not afraid of mosquitoes and the risk of Dengue, Chikungunga or Zika. We don’t have them and they never disturb our sleep. That is wonderful!!!

In fact, we feel safe here at high altitude and we avoid going to low lands as we don’t want to put our health at risk.
Homage to the work of the late Gustavo Zubieta-Castillo Sr.
If you missed it, you can read it here:
Interested in performing high altitude research?
Interested in performing research here in La Paz (3500m) in our labs at IPPA and/or Chacaltaya (5250m) at our pyramid laboratory two hours by car from La Paz? You could do it the week or two prior to the meeting. We will help you arrange it. A television network has expressed interest in recording this research at extreme altitudes.
Come join us and lets discuss all these concepts and many more. Express your ideas freely here in La Paz
See you in October.
Prof. Dr. Gustavo Zubieta-Calleja
High Altitude Pulmonary and Pathology Institute IPPA
High Altitude Pulmonary and Pathology Institute IPPA
www.Altitudeclinic.com
Rio Soqueri 55
Final Av.Saavedra,Prologanciòn Av. Copacabana
Map:
La Paz, Bolivia

The PanAm2014 Physiology Without Borders Conference

V Chronic Hypoxia Symposium news
Dear colleagues and hypoxia friends:
We will be hosting the V Chronic Hypoxia Symposium in Bolivia this October 6-11, 2014. Several outstanding scientists from around the globe will join us to discuss tolerance to hypoxia, and other aspects of hypoxia. Among them we have Jan Marino Ramirez, Robert Naejle, Frantisek Kolar, S.V Srikrishna, Wolfgang Jelkmann, Thuppil Venkatesh, Praveen Sharma, Jain Neera, and several other outstanding scientists. The setting is an itinerant symposium where we will carry out the conferences at different altitudes. If interested, please let us know. Our philosophy is that everyone can participate openly. Some months prior to the meeting we will post some questions regarding our themes at ResearchGate.net in order to carry out and develop a virtual discussion that will end at the meeting itself. All participants will be invited to post questions here (if they wish), prior to their presentation here in La Paz. This will certainly focus all of us on our subjects of interest in a dynamic way.
http://www/zuniv.net/symposium5
so, come join us!

V Chronic Hypoxia Symposium
Dear friends and colleagues around the world!
We are, once more, proud to announce the:
V Chronic Hypoxia Symposium
October 6-11, 2014Mark your calendar!

Uyuni Salt Lake 3
click here to go to the Symposium website
Colleagues from many countries in the world are enthused and lined up to honor us with their presence.
It will once more be an itinerant symposium, where talks are given in different altitude sites. We will visit and have conferences at:La Paz 3510 m
Titicaca Lake, 3800 m
Tiahuanacu ruins 4000 m
Chacaltaya at 5230 m
and the Salt Lakes 3656 m
You will learn of “life at high altitude” in different environments.
And this time we are going to visit the famous Salt Lakes at 3656 m in the South of Bolivia (shown above).
Click here to read more about the Uyuni Salt lakes.You will be completely impressed by the beauty of Bolivia and the hypoxic environment that is our “normal” everyday life.
click here to read about it.
During the V Chronic Hypoxia Symposium, we will have a meeting of the
International Society of Chronic Hypoxia.
It was created during the II Chronic Hypoxia Symposium
We will discuss about Life in Extreme Hypoxia and the
Tolerance to Hypoxia Formula.
Is it true that the paradox of going higher renders more tolerance to hypoxia?
Great scientists will join us in the analysis of these and other fascinating topics, so don’t loose the chance
by clicking here.
We are going to celebrate 44 years of scientific production in high altitude research..
Please read of our latest events and activities at:
http://altitudeclinic.com/blog/
All the best from Bolivia!!
Prof. Dr. Gustavo Zubieta-Calleja and Prof. Dr. Gustavo Zubieta-Castillo (Sr)….. still active
High Altitude Pulmonary and Pathology Institute
43 years of high altitude medicine
Web: AltitudeClinic.com
Email: zubieta@altitudeclinic.com
Phone: (591-2) 224-5394

The Lung at High Altitude
The Lung at High Altitude: From cellular acclimatization to clinical disease
August 3-7, 2012
Leh, Ladakh, J&K, India
Prior to the Global Hypoxia Summit and 4th International Conference on Chronic Hypoxia held in India, the Leh Symposium was carried out under the direction of Dr. Qadar Pasha, the organizing secretary that efficiently carried this meeting. We were invited speakers thanks to Dr. QadarPasha and substantially Prof. Thuppil Venkatesh.

It was an atmosphere of science and friendship, with pleasant discussions on the many aspects motivating the search for knowledge in hypoxia. Leh is located at 3500 m of altitude quite similar to La Paz. It is over an hour flight from Dehli. I understand there are 27 flights per day so it is a very popular tourist destination.
And of course, where you experience hypoxia. The Pulmonary Vascular Research Institute (PVRI) also participated as coorganizer. Likewise, the Institute of Genomics and Integrative Biology under the direction of Dr. Rajesh S. Gokhale, based in Dehli and the Sonam Narboo Memorial Hospital in Leh, J&K, India with Dr. Ghulam Mohammad. He kindly had us visit the hospital premises.

Several members of the PVRI were present including Ghazwan Butrous who recorded the conferences live and these will be available for the Fellows of the PVRI on their website. We again met Prof. Dr. Max Gassmann of the University of Zurich, Switzerland. He presented his work on Erythropoietin’ impact on exercise performance. Noteworthy was the presence of Dr. Sheila G. Haworth of the UK. She gave an intersting talk about surviving birht ath any altitude, Hypoxaemia to Normoxaemia. Prof. Thuppil Venkatesh, proposed a novel idea of gene mixing to improve human performance.

Robert Naejle from Universite libre de Bruxelles, was very inquisite and critical about the presentations, which gave it a stimulating touch, that we personally greatly enjoyed! He talked about pulmonary disffusion and exercise physiology. Jose Lopez-Barneo, from Spain gave an interesting talk about about the effects of chronic hypoxia on peripheral and central neurogenic centers. We also enjoyed the comments of Rubin Tuder from Denver Colorado. He talked about pulmonary vasculature and hypoxia signaling. Hari S. Sharma gave a brief talk on Angiogenensis and tissue remodeling. Dr. Gabriel Diaz from the Universidad Nacional de Colombia, in Bogota, talked about the hyperreactivity of the pulmonary vascular tree. Anita Saxena from the All India Institute of Medical Sciences talked about the Eisenmenger syndrome.

We also made good friends with Uttam Patti, from the Nehru University who was presenting interesting work on hypoxia in cancer cells. And we also were plesantly surprised by the presence of our bolivina colleague Alexandra Heath from Kardiocentrum in La Paz, Bolivia. Her work on neonatal pulmonary circulation at high altitude was also very novel. We also heard some talks on CMS from Dr. Prakash, Negi, Dr. Norboo Angchuk and Dr. Tsering Norboo.

Gustavo Zubieta-Castillo (Sr) gave a talk on Adaptation to life at the summit of Mt. Everest, adding new information to his hypothesis. Gustavo Zubieta-Calleja (Jr), gave a conference on a complete novel concept: The Tolerance to Hypoxia Formula, affirming that the higher one goes, the more tolerance to hypoxia there is.


The Global Hypoxia Summit & 4th International Conference on Chronic Hypoxia
At the High Altitude Pulmonary and Pathology Institute (IPPA) we had three previous successful meetings of Chronic Hypoxia in La Paz: http://zuniv.net/symposium/follow-up.html http://zuniv.net/symposium2/follow-up http://zuniv.net/symposium3/ During the second symposium the International Society of Chronic Hypoxia (ISCH), was created. Thanks to the coordination of Prof. Thuppil Venkatesh from St. John’s University in Bangalore, we have carried out under the direction of Prof. Shashi Bala Singh, Director of Defense Institute of physiology and Allied Sciences (DIPAS), in New Dehli, India 9-12 August,2012, the GLOBAL HYPOXIA SUMMIT & 4TH INTERNATIONAL CONFERENCE ON CHRONIC HYPOXIA.

This has been a conference of interesting, stimulating and excellent presentations and discussions in a most friendly manner and at the highest level in search for “Promoting Quality of Health in Hypoxia”. Noteworthy was the presence of his excellency the Minister of State for Defense – Government of India M.M. Pallam Raju, who personally attended the opening ceremony and impressed us with his know-how as he is an Engineer keenly interested in scientific matters. The video of Dr. Zubieta’s speech is here Dr. Shashi Bala Singh Director of Dipas, focused on 4 types of approach: Physiological, Nutritional, Herbal and Technological. A unique blend in search of excellence.

We, the Zubietas, had the pleasure of finding old friends such as Peter Bartsch, with whom we had spent wonderful moments, many years back during high altitude meetings and particularly one in Odessa, Ukraine when invited by a most disntinguished friend and colleague, Dr. Tatiana Serebrovskaya. We also met our dear friend Dr. Vidyasagar Casikar, We also had the please of establishing close friendship with Jan-Marino Ramirez, Nanduri R. Prabhakar, Benedito H. Machado. We also interacted with Hari S. Sharma, Akpay Sarybaev, Uttam Pati, Zahid Ashraf, T. Norboo, Col G. Himashree, Anju Bansal, Nazan Dolu, Praveen Vats, AK Salhan, and many others with distinguished scientific presentations.

The students also impressed us most favorably for the quality of their work, and we foresee an even greater scientific future for India. The scientific program can be found here. In the opening ceremony, Dr. W. Selvamurthy gave a most interesting work , with a resume of the scientific strategies used, based on research of the Indian Armed forces that perform operations at very high apoints including 6000m of altitude. He exclaimed “DRDO stands tall as a beacon for research in stressful environments in order to enhance the quality of life of the Man behind the Machine at high altitude”, a very stimulating and essential concept.

Dr. Shasi Bala Singh, in turn, commemorating the 50th anniversary of the Defense Institute of Physiology and Allied Sciences, in such an outstanding ocassion, expressed ” DIPAS has been working in the field of military physiology for the past fifty years with the primary mandate of promoting human performance in extreme performance”. From our point of view, this trip to India was extraordinary. The science, the friends, the philosophy, were all just great.

We would like to announce that the 5th Chronic Hypoxia International Conference will be held again in La Paz, Bolivia in October 2014. Please stay in touch for updates and development. Also, there will be a course on High Altitude Medicine, Physiology and Pathology on Feb-April 2013. Prof. Dr. Gustavo Zubieta-Calleja (Jr) and Prof. Dr. Gustavo Zubieta-Castillo (Sr)
