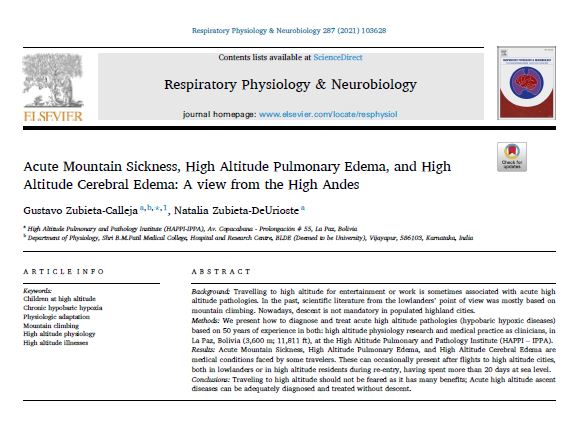
Much to many world scientists’ surprise, a group of sea-level “International high altitude experts” who defend a different point of view, wrote to the Chief Editor of the prestigious journal Respiratory Physiology and Neurobiology questioning our article: “Acute Mountain Sickness, High Altitude Pulmonary Edema, and High Altitude Cerebral Edema: A view from the High Andes” by Prof. Dr. Gustavo Zubieta-Calleja [his CV] and Dr. Natalia Zubieta-DeUrioste, published in Volume 287, May 2021 of the Respiratory Physiology & Neurobiology. Available as a Pre-print here. A full Journal printed scan version is available on request from the authors. Please send us an email.
The questions asked were properly answered with evidence-based medicine by the authors in a letter to the publishers. In order to find a solution, it was decided to stamp “RETRACTION” on the article (which would block the possibility of citations).
Interestingly, the same article received multiple congratulations and support. Simultaneously, the prestigious International Journal of Environmental Research and Public Health with an Impact Factor of 3.3 asked the author for an extension of the paper. Consequently, “The Oxygen Transport Triad in High-Altitude Pulmonary Edema: A Perspective from the High Andes” was published. In it, several of the questions are addressed.
Many scientists from around the world are giving their support asking for a NO RETRACTION of the paper, as any questioning should follow a standard course through a Letter to the Editor.
Some comments of support by very distinguished scientists of include:
Dear Gustavo
You have taken the right step for world scholars’ opinion to the journal.
I am always with you and will be.
It is disgusting to see some Western scientists’ attitudes towards Latin America and South Asian community fellow colleagues.
Science always prevails with experience, observation, and truth. Yes I agree that nothing is a universal truth in science and that is the beauty of science but ‘what I think is always right and there will not be any “alternate hypothesis” is a shallow mindset of a few people who never tested their own hypothesis in other environments.
Your research and honesty are beyond any doubt. You are not only a great scientist but also a great physician with credibility.
I did not find anything wrong or unscientific in this interesting thought-provoking research article with facts and deep logical analysis. To me, it is a great Science and I shall teach your alternate but strong theories and explanations to my University students without hesitations as a great novel contribution of high altitude biology.
I believe your work is a part of the progress of science for serving humanity!
I not only oppose the idea of this great publication retraction but also condemn it.
Regards
Kusal K.Das, PhD, FRSB
Distinguished Chair Professor in Vascular Physiology
Laboratory of Vacular Physiogy and Medicine
Faculty of Medicine
BLDE ( Deemed to be University ), Vijayapur,
Karnataka, India (560m)
Former Vising Professor
School of Medicine
University of Leeds, UK
( 2014 – 2016 )
Hony.Fellow
Karnataka Academy of Science & Technogy
Government of Karnataka
President
South Asian Association of Physiologists ( HO. University of Colombo ).
President’s message, above.
Member of International Union of Physiological Sciences (IUPS)
IUPS is the world body of physiologists with 84 countries and hundred societies
Dear Gustavo,
I fully support your publication. My details are as follows.
Prof. Praveen Sharma
PhD (Med), FACBI, FAMS, FAACC
Professor of Biochemistry,
(Former Head Biochemistry,
Dean (Research) & Controller of Examinations),
All India Institute of Medical Sciences,
Jodhpur-342005 ( India)
President ACBI (2003-2004 and 2014-2015)
President, InSLAR (2017 to date)
Chair, IFCC-CCLM (2020-to date)
Director, South East Asia on WASPaLM Board (2021 to date)
Editor-in-Chief, IJCB (2006 to date),
Chairman, APFCB Congress and Conferences (2019 to date)
Chairman, APFCB Communication committee (2010-2019)
Chief Editor, APFCB News (2010-2019)
Director, NRCLPI, Jodhpur (2014 to date)
Assessor (NABL )
International Lead Assessor (AERSSC)
Mobile:+91-8003996869
+91-9414044562
Email: praveensharma55@gmail.com
sharmapr@aiimsjodhpur.edu.in
Someone has to pioneer the road to higher consciousness through scientific exploration. You have. Your paper is stellar and ahead of its time.
There was a saying in the 1960s I abide by: “keep on keeping on.”
Be proud of your forward-thinking ideals. Westerners will catch up to you in time.
Dr. Kathryn Rossie, PhD
Clinical Psychologist
Researcher
Author, Publisher, and Editor
Consultant: International level. Private Practice Consultation: California.
Professor of the Neuroscience Institute for Psychotherapists of San Lorenzo Maggiore, Italy.
Chief Financial Officer (CFO) and Vice President:
The Ernest Lawrence Rossi Non-Profit Foundation for Psychosocial Genomics Research
Board of Directors: The Milton H. Erickson Foundation Press
Founding Director of the Milton H. Erickson Institue of the California Central Coast (MHE-CCC)
All high altitude researchers in India including HPRC (High Altitude Physiology Research Cell, Darjeeling), high altitude research facilities St John’s team, Defense Institute of Physiology and Allied Sciences (DIPAS) are all in support of the research paper published by Professor Gustavo et al. We require scientific community to take this concept forward without any bias and come out with the most appropriate guidance documents to manage chronic Hypoxia.
With regards,
Dr Thuppil Venkatesh
President
International Society of Chronic Hypoxia
CEO and Director
Chairman Indian Society for Lead awareness and research and
Director
The National Referral Center for Lead Poisoning Prevention in India (NRCLPI)
Foundation for Quality India (FQI)
The Lead Man of India
Professor Emeritus
Biochemistry Department St John’s Medical College
Bangalore, India
Dear Gustavo,
Thank you for the materials you sent me. I need some time to study these materials more closely, delving into the arguments and comparing them.
Being a specialist in some intracellular molecular mechanisms of adaptation to hypoxia, I will not take the responsibility to take part in the discussion on issues of respiratory physiology and practical medicine.
However, in any case, I consider the precedent of retraction of the already published article extremely dangerous. This not only destroys constructive scientific discussion, based on the freedom of publication by each of the side of its position and arguments. This also threatens us with an Orwellian dystopia of an unpredictable changing past. This precedent is especially dangerous in conditions when more and more scientific journals have only an electronic version and are not published in paper form. With this approach, we can get a situation where, with each change of the prevailing concepts in science, articles previously published in electronic journals will “disappear” as if they never existed.
Of course, I join to letter to the Chief Editor and Publishers asking for NO RETRACTION.
Sincerely,
Dr. Sergei Alexandrovich Stroev, PhD
I.P. Pavlov Institute of Physiology of Russian Academy of Sciences, Russia (2000-2015), University of Tampere, School of Medicine, Finland (2001-2014).
P.S. By the way, I was somewhat surprised by point 4 of your opponents’ objections, where they state: «“adaptation” must be limited to genetically transmissible changes because they are integrated into the gene pool of a particular population or species».
My thesis, which I successfully defended in University of Tampere was called “The role of endogenous protein antioxidants in neuronal adaptation to hypobaric hypoxia”.
https://trepo.tuni.fi/bitstream/handle/10024/95013/978-951-44-9354-6.pdf?sequence=1&isAllowed=y
The dissertation dealt with adaptation to hypoxia of cells and the organism as a whole at the level of regulation of the expression of individual proteins without any genetically transmissible changes (I will not vouch for epigenetic changes in this model – I have not studied this issue). And the term “adaptation” in this sense of an individual, not related to genetic changes, adaptation did not cause any objections from highly professional opponent, reviewers and many specialists who were present at the defense of the thesis.
Many other authors use this term in the same meaning, for example:
Samoilov M.O. Brain and adaptation. Molecular and cellular mechanisms. St. Petersburg,
1999. 272 p. (In Russian).
Portnichenko V.I., Nosar V.I., Sydorenko A.M., Portnichenko A.H., Man’kovs’ka I.M.
Continuous adaptation of rats to hypobaric hypoxia prevents stressor hyperglycemia and optimizes mitochondrial respiration under acute hypoxia. Fiziol Zh. 2012 b. 58(5): 56-64 (In Ukrainian, summary in English).
Meerson F., Pozharov V., Minyailenko T. Superresistance against hypoxia after
preliminary adaptation to repeated stress. J Appl Physiol. 1994. 76(5): 1856-1861.
Lukyanova L.D., Sukoyan G.V., Kirova Y.I. Role of proinflammatory factors, nitric
oxide, and some parameters of lipid metabolism in the development of immediate adaptation to hypoxia and HIF-1α accumulation. Bull Exp Biol Med. 2013. 154(5): 597-601.
Lu G., Ding D., Shi M. Acute adaptation of mice to hypoxic hypoxia. Biol Signals Recept. 1999. 8(4-5): 247-255.
49 world distinguished scientists have supported the quality of this article. We are most thankful !

 The original article was printed in the Volume 287, May 2021 of the Respiratory Physiology and Neurobiology journal
The original article was printed in the Volume 287, May 2021 of the Respiratory Physiology and Neurobiology journal

The link to this article is:
https://www.degruyter.com/document/doi/10.1515/reveh-2021-0172/html