CASE # 6081
Dear prestigious colleagues:
Thank you once again for your important contributions. The Learn and Teach series was named so because medicine is a complex subject. As true scientists, we are always near the absolute truth, but never there.... Medicine is a dynamic science with permanent evolution of knowledge. We have all learned and taught. Controversies are helping us grow.
Please note that in this section, we answer questions addressed to us, in italics.
POST FOLLOW UP
Click on the links below to see their comments.
John Severinghaus
Pr. Jean-Paul Richalet
Tom Hornbein
Dr. Thuppil Venkatesh
Univ.Prof.Dr.Franz Berghold
--------------------------------------------------------------------------------------------------------
You write: His chest x-rays were also atypical
of HAPE. The edema was centrally located near the mediastinum, which probably
explains absence of abnormal breath sounds".
In my experience, that is the typical locus for appearance of HAPE, and
it was that
observation in the 1960s by others that led me
to wonder if the leak is due to overexpansion of the pulmonary arteries
by the
constriction of the precapillary sphincters,
and resulting rise in PAP. That concept fits all the observations
better than any other
theory of site of leak and its cause.
Another example is unilateral HAPE or more correctly pulmonary edema when
surgeons do a
Potts and shunt arterial blood into the pulmonary
artery of kids with pulmonary atresia. Edema occur near the anastomosis.
I
suspect it also underlies the sudden edema in
strong young men whose airway obstructs after surgery when an endotracheal
tube is
remove. They fight for breath, get no air,
Po2 plummets, PAP rises abruptly, with high cardiac output, and PA is overdistended.
Heroin PE may be similar, apnea plus sympathetic
nervous hyperactivity, the high.
Regards
John
--
John and Elinor Severinghaus
PO Box 974, 20 Allen Ave
Ross CA 94957
415-456 4593
Dear John:
Very interesting and important comments. We are happy to know this case report supports your previous observations.
Gustavo Sr. and Gustavo Jr.
Back to top
-----------------------------------------------------------------------------------------------------------------
Interesting observation, but I don't understand
a few things:
1. why is it atypical ? It looks to me very similar
to usual cases. You can see HAPE in the Alps at lower altitudes than la
Paz.
Dear Jean Paul:
This case was different to others we commonly observe, like the ones below.
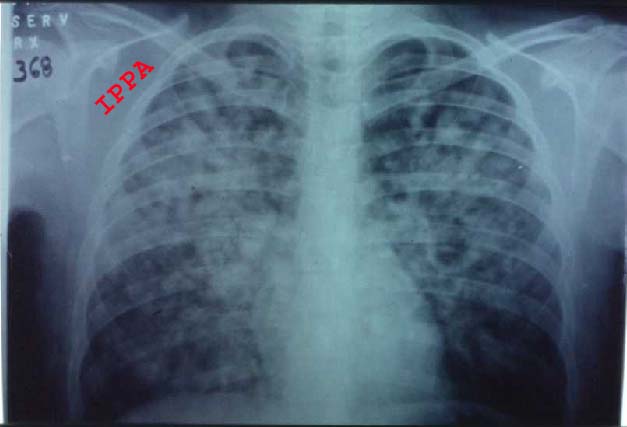
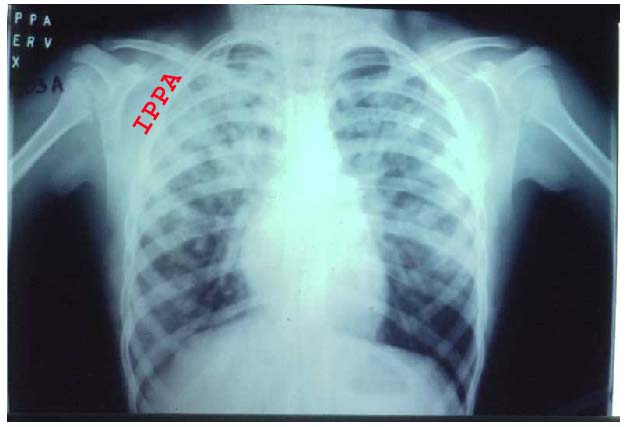
It was associated to an abnormal ecg (please note that the tachycardia continued for a while even after the edema was resolved) and systemic hypertension . It looks like that in some aspects, we have different experiences, or lack of information. We will appreciate it if you can send us a chest xrays similar to this one for comparison. Also, please specify the altitude at which it was taken. This because we observe full blown HAPE with peripherally located infiltrates and of course abnormal breath sounds and blood stained sputum. Perhaps, we used the term "atypical" inadequately ?
2. Overweight is a risk factor, due to hypoventilation
We agree.
3. Why this patient was not treated by usual recognized
treatment of HAPE (calcium blockers ?) but by digoxin, since we know that
heart is not a problem in HAPE ? And why antibiotics
?
We don't use calcium channel blockers for HAPE, and we think Venkatesh (below) has an opinion regarding this. Digoxin is in fact not used in HAPE, and we don't advice its regular use. But in this case we did, because he had tachycardia, had an abnormal ecg showing inotropic alterations and was given oxygen therapy, which is the best treatment for pulmonary hypertension at high altitude. Since no massive pulmonary edema was present, digoxin did in fact help. His recovery was prompt.
Why antibiotics ? Perhaps you missed the first communication where we report 13,700 WBCs. Also, we and others have previously reported that in pulmonary edema, there is always an inflammatory compromise. In children, virus seem to play an important role. In adults, bacteria have been associated to HAPE in a case report where we isolated Streptococcus Pneumoniae, as published at:
Gender differences in CMS (published in Japan)
In the present case we couldn't isolate the
bacteria due to time constraints. Joe
Fischer has the same opinion.
Best wishes
Pr Jean-Paul Richalet
Back to top
----------------------------------------------------------------------------------------------
Fascinating and curious case and beautifully presented to us.
Much best to you and your families.
Tom Hornbein
Back to top
---------------------------------------------------------------------------------------------
Dear Professor and other Friends,
It is a wonderful experience to have interacted
with so many like mined people concerned about the high altitude problems.
Hope to
meet you all in China during the World Congress
hosted by Professor Ge Ri-Li. We can also think of having a session exclusively
for
the case discussion. Thanks to Professor Gustavo
Zubieta. I love to meet you all and I am sure that the same with
you. I had an
opportunity to visit IPPA in La Paz. I found
the altiplanoes much similar to Tibetians and sherpas.
I do wonder if the interesting cases selected
could be published which will remain as a guidelines and will also show
us the trend in
the clinicians concern in treating the cases
of problems caused at high altitudes with growing concern about the recent
trends in the
advances in treatment. Newer drugs and medicines
have been used and more complicated cases are diagnosed with laboratory
support and portable field POCT. We have challenges
ahead of us and we do have knowledge accumulated to create sufficient
confusion. All should ultimately lead to simple
non invasive inexpensive treatment protocol to help the sick.
With best wishes, Thanking you all once again.
Dr. Thuppil Venkatesh
Back to top
---------------------------------------------------------------------------------------------
Dear Gustavo,
many thanks - I am looking forward to the next
case report.
Kindest regards,
Franz
Univ.Prof.Dr.Franz Berghold
Präsident der Österreichischen Gesellschaft
für Alpin- und Höhenmedizin
A-5710 Kaprun 130
Tel +43/6547/8227 Fax +43/6547/7772
Email: bergi@eunet.at
Homepage der Österreichischen Gesellschaft
für Alpin- und Höhenmedizin: www.alpinmedizin.org