Case # 6081
We want to thank everyone for the very interesting
comments
(click here to see them) on this case . Below we present a description
of
Clinica IPPA´s follow-up with the patient
in this case study.
FOLLOW UP:
Based upon the test results we outlined in our
initial presentation, the patient was hospitalized at IPPA, with the diagnosis
of HAPE, and
right heart failure. He was administered
100 % oxygen by mask at a flow 3 liters per minute, he was monitored,
and given antibiotics,
electrolytes, digoxin and bed rest. The following
day he was placed in the hyperoxic/hypoxic
adaptation chamber for three hours
breathing a PIO2 of 150 mmHg. His tachycardia
of 120 bpm gradually declined to 100 bpm. The patient felt much better
and
recovered his appetite.
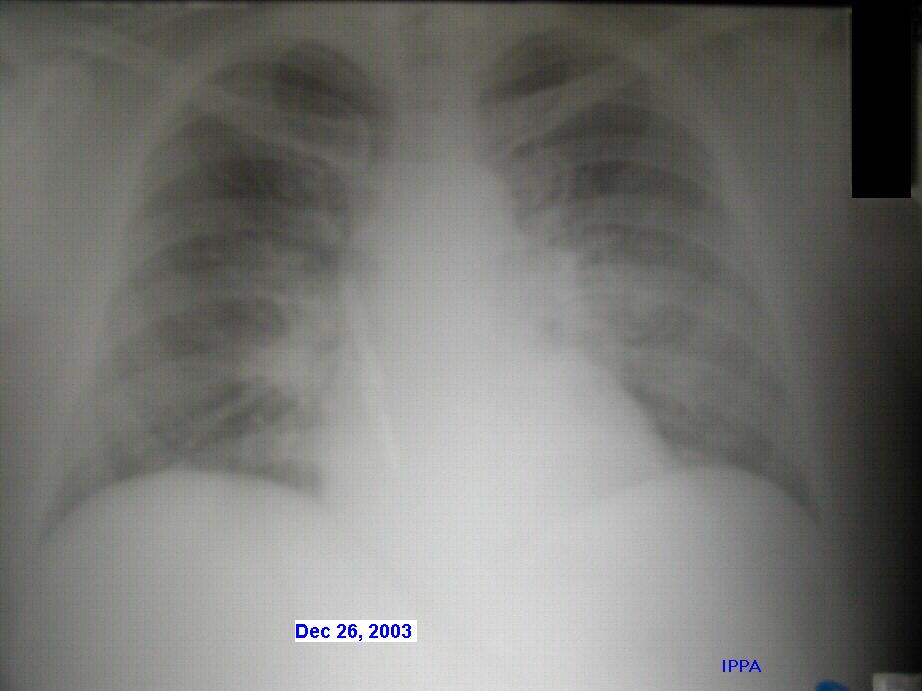
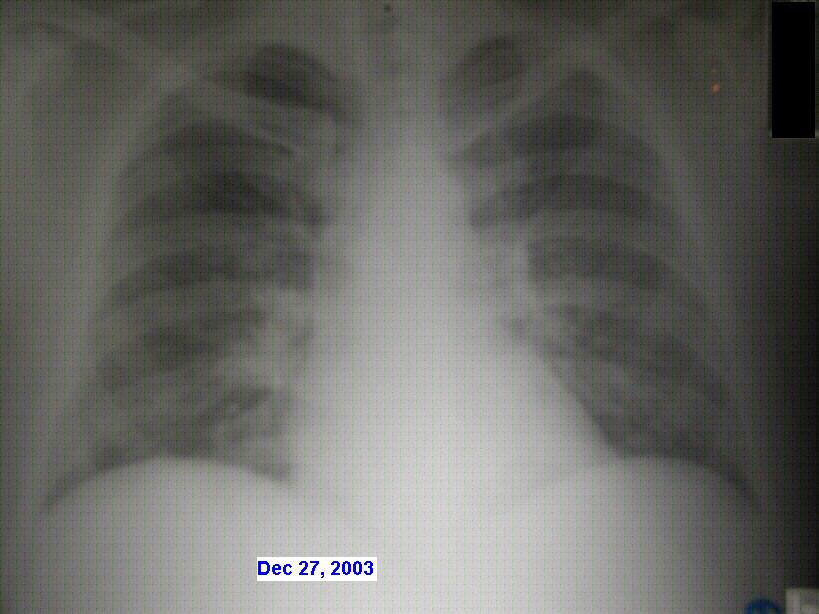
The chest x-rays on day 2 [click on the link to view the x-rays] showed clearing with respect to the previous chest x-ray. A follow-up
The patient felt so well by the end of the day
two, that he asked to be discharged, even though one more day of hospitalization
was
advised. He returned to the clinic two days later
feeling normal. Seven days later a chest x-ray and ecg (taken elsewhere)
revealed no
abnormal findings, with the exception of
the tachycardia and slight systemic hypertension.
DISCUSSION:
This case shows that HAPE does not always follow
the classic patterns of the disease due to high altitude ascent, in this
case to the
altitude of the city of La Paz at 3600 m with
no further ascent. The disease developed gradually over four days and was
being
considered as a routine mild AMS. However deterioration
was gradual and slow due to intermittent oxygen administration. This is
an
overweight patient, who used chemical substances
to clean car tires and used no respiratory protection during many years.
His chest
x-rays were also atypical of HAPE. The edema
was centrally located near the mediastinum, which probably explains absence
of
abnormal breath sounds. Prompt recognition before
a full blown HAPE is established also suggests this is how many cases of
HAPE
begin. The ecg was in fact abnormal with
notching in the QRS segment in II, III and V-5, V-6 and T axis clockwise
rotation in pre
cordial leads, that was interpreted as RV strain.
The hyperglycemia seems to be stress related. He has a tendency to systemic
hypertension that will probably require permanent
treatment at sea level.
-----------------------------------------------------------
We hope you have enjoyed giving this case report
your consideration -- this case will remain open for discussion and further
comments
are welcome. This series is open-to-all who wish
to participate. Brief or extended comments, suggestions and opposing viewpoints
are
always invited..
More case reports will follow -- please
let us know if you would like to remain on our distribution list, and do
not hesitate to invite
others to join in. Have a nice and lovely day
and best regards from Clinica IPPA!
Prof. Dr. Gustavo Zubieta-Castillo
(Sr) &
Dr. Gustavo Zubieta-Calleja
High Altitude Pathology
Institute (IPPA)
Further comments of the POST-FOLLOW-UP section can be found here
{kind=link}
{kind=link}