El uso de la palabra polieritrocitemia creado por el Prof. Dr. Gustavo Zubieta-Castillo se esta generalizando.
Los Doctores Gustavo Zubieta-Castillo y Gustavo Zubieta-Calleja fueron invitados a participar en el 6to Seminario Internacional de Salud Ocupacional en operaciones mineras llevado a cabo el 23 y 24 de octubre de 2014, en Lima, Peru. En esa oportunidad el Dr. Zubieta-Castillo hablo sobre la polieritrocitemia, sus causas y sus tratamientos. El Dr, Zubieta-Calleja habló sobre la hipoventilacion en la altura y sus efectos.
Una disertación en la Universidad Nacional de Cajamarca para el titulo de Médico Cirujano:
Instituto Pulmonar y Patología en la Altura (IPPA)
English version below
Nuevamente estamos en Octubre, cuando nuestros cielos se llenan de rayos solares maravillosos en toda Bolivia, pero…. ¿Chaqueos de nuevo? ¿Humo de nuevo? ¿Ciudades con el aire contaminado?
Este planeta es hermoso. Es el producto estrella del Universo. Todavia no hemos descubierto la vida fuera del planeta. ¿Se dan cuenta todos lo extraordinario y fantastico que esto es?
La tecnologia y la ciencia han avanzado a grandes pasos, sin lugar a duda. Los celulares, las computadoras, el vuelo, incluso el ir a la Luna. Notables logros de la inteligencia, la tenacidad, el esfuerzo de grandes hombres. Pero esos logros en perspectiva, son infinitesimalmente insignificantes, frente a la grandeza de la naturaleza. Uno de los elementos mas esenciales de la vida, es el oxigeno. Los humanos, los seres vivos, mas inteligentes del planeta, y quizas, aunque suene demasiado audaz, de todo el Universo, necesitamos de este precioso elemento: el oxígeno. Curiosamente, el oxígeno que respiramos, no fué producido en la tierra. Lo fabricaron grandes explosiones en el espacio. La tierra fue la ganadora de la loteria de su distribucion y su mezcla con temperaturas adecuadas, y otros elementos vitales. Llego atravesando espacios casi ilimitados para posarse en un planeta donde tambien hay agua, y todos los otros elementos preciosos de la vida. Pero es el oxigeno, el mas vital, por ser el que no puede ser guardado en el organismo. Podemos dejar de comer solidos y sobrevivir hasta un mes, dejar de ingerir liquidos y sobrevivir 1 semana. Pero dejar de respirar e inhalar el oxigeno solo podemos hacerlo unos 3 a 5 minutos. Si no ingresa a los pulmones el aire con 20.9% de oxigeno, estamos frente a la muerte. Es por eso que este elemento precioso, no tiene precio. Vale mas que el oro, pues el Coronavirus lo ha demostrado ampliamente. Podria ser el hombre mas rico, pero si no entraba suficiente oxigeno a la sangre para nutrir a los tejidos y a nuestro cerebro, todo se acabó. Es el fin a pesar de estar hechado en una cuna de oro.
Como médico especialista en medicina de la altura y habiendo trabajado durante 50 años a lado de mi Padre el Prof. Dr. Gustavo Zubieta-Castillo fundador de el Instituto Pulmonar y Patología en la Altura (IPPA), considero mi apremiante responsabilidad dar los mas importantes y urgentes consejos.
Desde el inicio de la Pandemia en Wuhan, China, me he visto atrapado como en una avalancha dedicando mi atencion y todos mis conocimientos, a lado de mi hija Natalia, medico de profesión al frente de batalla creado por este terrible Coronavirus-2 que desencadena la enfermedad denominada COVID-19. Recibi una gentil invitacion para participar en un programa radial sobre el Coronavirus en Enero de 2020. Mi primera reaccion fue la de rechazar la invitacion porque afirmé que yo no era epidemiólogo y realmente no sabia mucho de esta enfermedad, “colgando” así el teléfono. 5 minutos transcurrieron y volvieron a llamarme. Nuevamente escuché la amable voz de Jackeline Barriga, quien habiendo comunicado mi decision a Johny Villaroel gestor de la invitacion y director del programa Desarmado Discursivo, me decia que realmente querian que participara y diera mi opinion. Aparentemente, una previa entrevista en la radio de la UMSA, le habia agradado y sentía que yo deberia participar, junto al Dr.Nestor Taboada, el otro entrevistado. Reflexionando, acepté y ello cambio el curso de mi atencion y enfoqué todos mis esfuerzos a entender mejor a este tremendo virus con el único objetivo de salvar vidas.
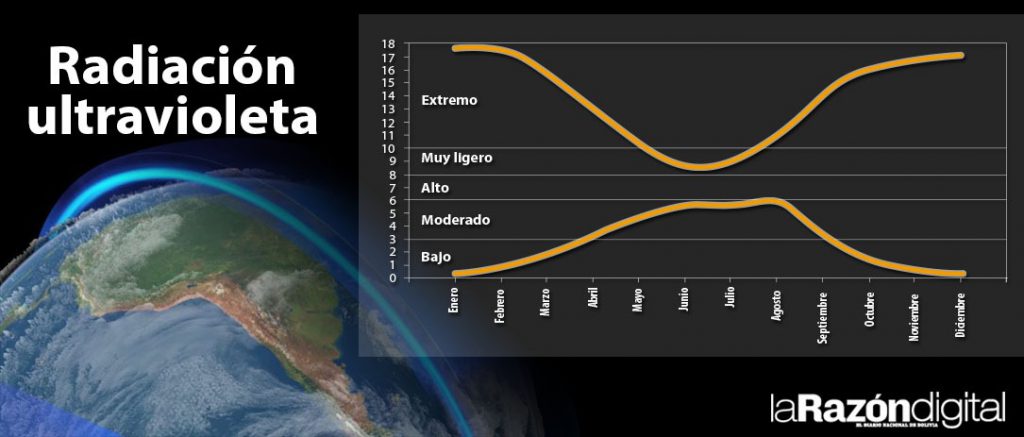
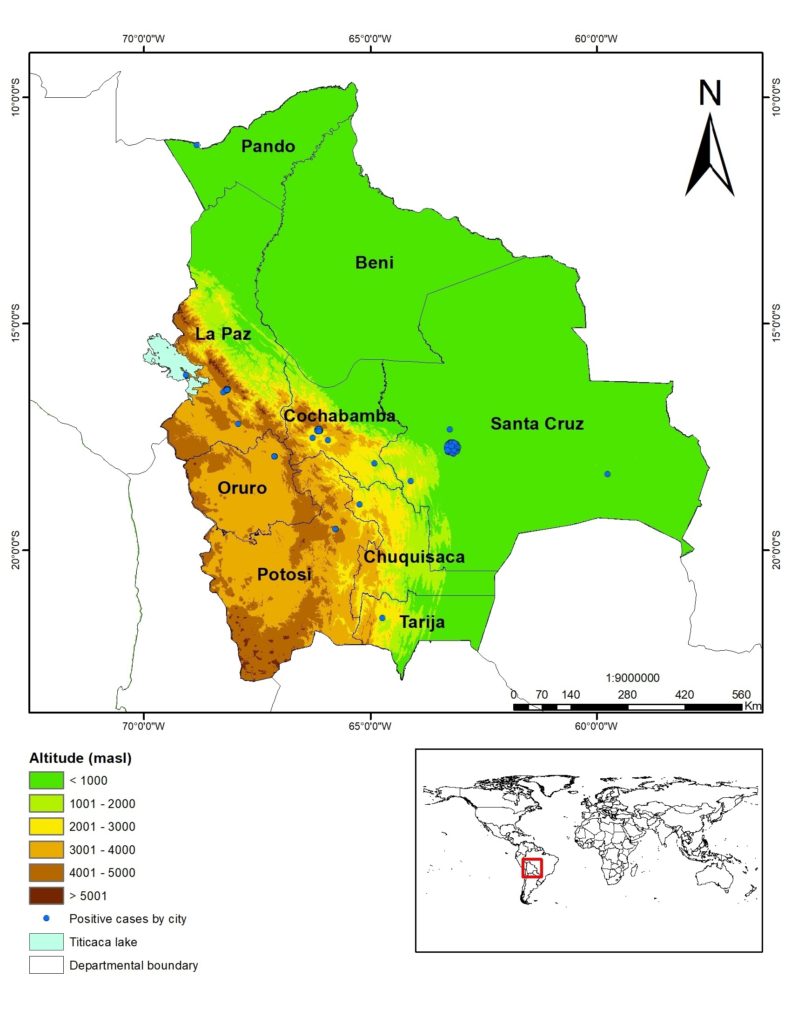
En vivo, propuse la idea, de que las personas infectadas que llegaran al aeropuerto de La Paz, deberian ser aisladas en un reciento alejado de la ciudad y en el altiplano para evitar la progresion de la enfermedad. Ademas aduje, que la radiación ultra-violeta que se encuentra en niveles extremos en la altura, seria una ventaja frente al Coronavirus. Esa ultima afirmacion, basada en el concepto de las ventajas de la radiacion ultra-violeta en la altura como anti-baceriano, la había hecho 2 años antes en una publicación donde demostraba la longevidad extendida del hombre en la altura, comparada con los habitantes del llano, basado en un estudio de datos provistos por el SEGIP (https://www.zuniv.net/pub/Longevidad_Espanol.pdf). Posteriormente el 5 de Abril, 2020 publiqué un articulo en La Razón, en Marzo, donde afirmé que la radiación ultra-violeta nos protegería del COVID-19. Y evidentemente la progresion fue mas lenta en la ciudad de La Paz y el Alto inicialmente. Sin embargo, en Julio hubo un incremento importante de casos, que de todas maneras no llegaron nunca a sobrepasar los de Santa Cruz, aunque ambos departamentos cuentan con un numero similar de habitantes (La Paz, 2.9 M y Santa Cruz 3.37 M). Este incremento se dió porque en invierno la radiacion ultra-violeta está en su punto más bajo. Pero luego del solsticio de invierno, gradualmente fue aumentando la radiacion ultravioleta y concomitantemente empezaron a disminuir los casos de COVID-19, como vaticinamos. La incidencia de la mortalidad también es más baja en la altura, como lo confirmamos con el Dr. Freddy Armijo Subieta en varias oportunidades. La altura, sin duda alguna, es un protector contra la agresividad del Coronavirus, no solo por las caracteristicas ambientales, sino tambien por las caracteristicas biológicas de adaptación a la altura. Publicamos varios articulos científicos en revistas internacionales al respecto.
Cuando las publicaciones del exterior afirmaron que en Nueva York, en los hospitales mejor equipados del mundo, la mortalidad de los que estaban con ventiladores era de 88.7%, me pregunté: que esta ocurriendo en los pulmones con la agresion de este virus? Inmeditamente, me dí cuenta que no estabamos frente a una neumonia típica tipo SARS, como aducian los expertos de todo el mundo. Estabamos frente a una nueva enfermedad. Desarrollé la idea nueva para todo el mundo, de la neumólisis, la destruccion de los pulmones ocasionada por el virus. Lo mencioné por primera vez en la primera conferencia del Coronavirus en la India, donde fuí invitado a participar y colaboré activamente invitando a otros colegas. Se lo mencioné al profesor Italiano Paolo Pelosi autoridad mundial en ventilacion mecánica. El habia tratado a multiples pacientes en las unidades de trapia intensiva en toda la catastrofica pandemia en su país y todavia no comprendian claramente que ocurria. El 9 de Julio,2020 (coincidiendo con el 50 anniversario del IPPA) el periodico El Diario me hizo una entrevista y alli hable en Bolivia por primera vez de la Neumólisis. Luego fuí invitado a ser co-director del 2do Congreso mundial de Avances en el COVID con el Prof. Malali Gowda del Bangalore Genomics Center en la India. Llevamos a cabo dicho exitoso evento del 27 al 30 de Agosto, 2020 con presencia de grandes científicos como el Dr. Andrew Pollard, un amigo, director de la Vacuna de Oxford, y el Dr. Robert Gallo, uno de los descubridores del virus del SIDA, entre otros notables cientificos, a quienes invité. Allí expuse en más detalle la Neumólisis y la hipoxia silenciosa (baja del oxigeno), que puede llevar a la muerte subita. Hablé no solo de los estudios microscopicos sinó de la fisiopatologia de esta terrible enfermedad. El Prof. Pelosi presentó pruebas adicionales de la neumólisis, confirmando su existencia. Lo invité a dar con mi persona, 2 conferencias aquí en La Paz. Tambien publicamos con mi hija Natalia, sobre la neumólisis en el Boletin Nacional de Bioetica, dirigido por el Doctor Javier Luna Orozco.
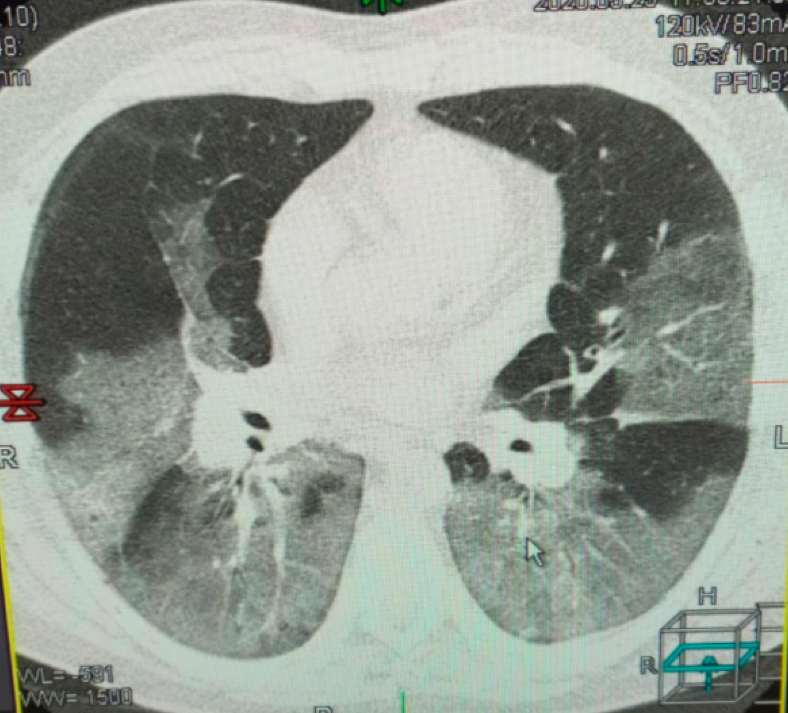
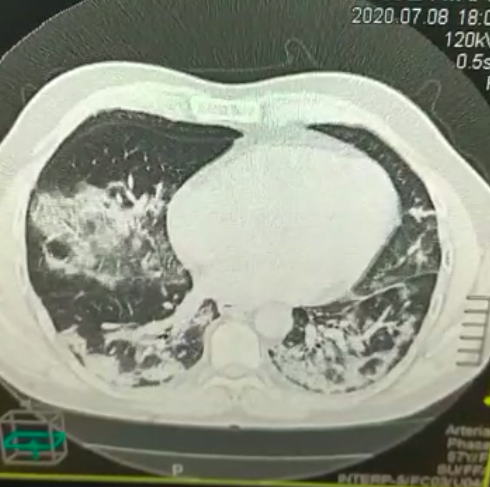
El nuevo concepto “Neumólisis” desarrollado por mi persona, en referencia al compromiso serio ocasionado por el Coronavirus en la actual pandemia del COVID-19, se constituye en un factor de gran riesgo en esta epoca. El Coronavirus ingresa al pulmón por via inhalatoria y se anida ingresando por los receptores ACE-2 en los neumocitos (las celulas respiratorias en el pulmón), el material RNA del virus se reproduce y ocasiona la destrucción de estas celulas: Neumólisis (neumo=pulmón, lisis=destrucción).
neumólisis en COVID-19
Es por eso que se produce una lesión severa de diversas partes del pulmón (zonas blancas en la tomografía), ocasionando un descenso del nivel de oxígeno, evidenciado por el pulsoximetro digital. Los pulmones de los pacientes se van destrozando gradualmente conforme el virus se propaga y llegan a producir la “hipoxemia silenciosa o silente”. Hipoxemia (hipo=baja,oxemia=oxígeno en la sangre) que se mide con el pulso-oxímetro.
Volviendo a los chaqueos, en estas circumstancias el humo en el ambiente, es un factor seriamente agravante compromitiendo la salud, particularmente de los que no tienen acceso al oxígeno medicinal, lo que puede costarles la vida. El humo, además bloquea el ingreso de la luz solar, y por lo tanto, la radiación ultra-violeta que nos protege del coronavirus como lo afirmé en el articulo: Las ventajas de la radiacion ultra-violeta en el control del coronavirus en la altura (La Razon, 5 de Abril, 2020). Y recientemente a sugerencia del Físico Roberto Vera, lo analizamos en el Boletín: https://zuniv.net/pub/BOLETIN1Ambiente_13oct.pdf.
Los que logran sobrevivir al ataque del virus, se recuperan pero pueden quedar con un cuadro de fibrosis (cicatrización) pulmonar severo que disminuye la captacion de oxigeno y reduce su capacidad para hacer ejercicio. Es decir, quedan los pulmones con limitaciones. Ante estas circumstancias de insuficiencia respiratoria, el humo ocasionado por las quemas, es un factor seriamente agravante, que pone en riesgo la vida de los habitantes.
Mas aún, los pulmones de la naturaleza, son las plantas y los arboles que a traves de sus hojas y por la acción de los rayos solares generan el oxígeno en el planeta, a traves de un ciclo de metabolismo celular. Al destrozar estos “pulmones de la naturaleza”, por la quema, tambien se ve seriamente comprometido el medio ambiente de todo el planeta. Practicamente, todos los animales del planeta necesitan el oxígeno para sobrevivir. Es por eso que al igual que lo que se ha denominado Neumólisis a nivel pulmonar (de un micro-ambiente en nuestro cuerpos), debemos denominar Forestalisis (forestal=bosque, lisis = destrucción), Forestlysis en Inglés, a la destrucción de las plantas por la quema (de el macro-ambiente). Lo que, a su vez conlleva al compromiso de no solo la flora, sino también la fauna por agresión directa de las quemas y por la ausencia de fuentes de alimentación en base a plantas. FOTO (PERIODICO OPINION, 19 DE JULIO 2011)
En el COVID-19 el coronavirus destroza el pulmón del ser humano (Neumólisis) y produce la muerte. En los chaqueos (quema de los bosques) el ser humano destroza el pulmón de la naturaleza (Forestalisis). Esos irresponsables que prenden fuegos, son los “virus del planeta” y los que van a destrozarlo. Y de esta manera es un suicidio global comprometiendo nuestras vidas, todas nuestras plantas, todos nuestros animales, todo, absolutamente toda……… la vida!!!! Es por todo esto, ciudadanos bolivianos y de todo el mundo, que debemos dejar de producir chaqueos incontrolables, porque estamos hiriendo severamente a la madre tierra y esta Forestalisis (nuevo termino que invento), puede llevar a nuestro planeta a un éxito letal donde todos y cada uno de nosotros perderemos la más valiosa joya del universo: La vida!
Pulmonary Institute and Pathology at Altitude (IPPA)
We are again in October when our skies are filled with extraordinary solar rays throughout Bolivia, but…. ¿ Forest burning again? ¿ smoke again? Cities with polluted air? This planet is beautiful. It is the star product of the Universe. We have not yet discovered life outside the planet. Does everyone realize how extraordinary and fantastic this is? Technology and science have made great strides, without a doubt. Cell phones, computers, flight, even going to the moon. Remarkable achievements of intelligence, tenacity, the effort of great men. Nevertheless, those achievements in perspective, are infinitesimally insignificant compared to the greatness of nature. One of the essential elements of life is oxygen. Humans, the most intelligent living beings on the planet, and perhaps, although it sounds too daring, the entire Universe, we need this precious element: oxygen.
Interestingly, the oxygen we breathe was not produced on earth. Great explosions made it in space. The land was the winner of its distribution lottery and its mixture with suitable temperatures and other vital elements. It came through almost unlimited spaces to land on a planet with water, carbon, and all the other precious elements of life. However, oxygen is the most vital element, as it cannot be stored in the body. We can stop eating solids and survive for up to a month, stop drinking liquids, and survive one week. Nevertheless, to stop breathing (and inhaling oxygen) can only be done for about 3 to 5 minutes. If the air with 20.9% oxygen does not enter the lungs, we are facing death. That is why this precious item is priceless. It is worth more than gold because the coronavirus has amply demonstrated it. One could be the richest man on the planet, but if enough oxygen did not enter the blood to nourish the tissues and our brain, it was all over. It is the end despite being cast in a cradle of gold.
As a specialist in altitude medicine and having worked for 50 years alongside Father, Prof. Dr. Gustavo Zubieta-Castillo, founder of the Pulmonary Institute and Pathology at Height (IPPA), I consider it my pressing responsibility to give the most critical and urgent advice. Since the Pandemic in Wuhan, China started, I have been caught, as if in an avalanche, dedicating attention and all knowledge with my daughter Natalia, a doctor by profession at the scientific forefront created by this terrible Coronavirus-2 that triggers the disease called COVID -19. I received a kind invitation to participate in a radio program about the Coronavirus in January 2020. My first reaction was to reject the invitation because I affirmed that I was not an epidemiologist and I really did not know much about this disease, so I rejected the invitation and hanged up. Five minutes passed by, and they called me again. Again I heard the gentle voice of Jackeline Barriga, who had communicated my decision to Johny Villaroel, manager and program director Desarmado Discursivo. They again asked me to participate and give my opinion. A previous interview on the UMSA radio had pleased him, and he felt that I should participate, along with Dr. Nestor Taboada, the other interviewee. Reflecting, I accepted and changed the course of my attention and focused all my efforts to understand this terrible virus better to save lives.
The altiplano and Mt. Sajama
On the air, I proposed the idea that people infected with COVID-19 arriving to the airport of La Paz should be isolated in an adapted building away from the city and the altiplano. This, to prevent the progression of this terrible, highly transmissible disease. I also argued that ultraviolet radiation found at extreme levels at altitude would be an advantage over the coronavirus—that last statement, based on the concept of the advantages of ultraviolet radiation at high-altitude as anti-bacterial. This was exclaimed two years before, in a publication demonstrating the extended longevity of man at high-altitude, I compared to inhabitants of the lowlands, based on a study of data provided by SEGIP ( https://www.zuniv.net/pub/Longevidad_Espanol.pdf ).
Later on April 5, 2020, I published an article in La Razón in March, where I stated that ultra-violet radiation would protect us from COVID-19. As expected, the progression was slower in La Paz and El Alto initially. However, in July, there was an essential increase in cases, which in any case never reached those of Santa Cruz, although both departments have a similar number of inhabitants ( La Paz, 2.9 M and Santa Cruz 3.37 M ). This increase occurred because, in winter, ultraviolet radiation is at its lowest point. However, after the winter solstice, the ultraviolet radiation gradually increased, and concomitantly the cases of COVID-19 began to decrease, as we predicted. The incidence of mortality is also lower at altitude, as we confirmed with Dr. Freddy Armijo Subieta on several occasions. Without a doubt, high altitude is a protector against the coronavirus’s aggressiveness, not only due to environmental characteristics but also due to the biological characteristics of adaptation to high-altitude. We published several scientific articles in international journals on the matter. When the foreign publications stated that in New York, in the best-equipped hospitals globally, the mortality of those with ventilators was 88.7%, I asked myself: what is happening in the lungs with the aggression of this virus? I immediately realized that we were not facing a typical SARS type pneumonia, as experts from all over the world adduce. We were facing a new disease. I developed a new concept for everyone, pneumolysis, the destruction of lungs caused by the virus. For the first time at the first Coronavirus conference in India, I mentioned it where I was invited to participate and actively collaborated by inviting other colleagues. I mentioned the idea to the Italian intensivist Paolo Pelosi world authority on mechanical ventilation, during the conference on COVID-19 in India. He had treated multiple patients in intensive care units throughout the catastrophic pandemic in his country, and they still did not clearly understand what was happening. On July 9, 2020 (coinciding with the 50th anniversary of the IPPA), the newspaper El Diario interviewed me, and there I spoke in Bolivia for the first time about the Pneumolysis. Then I was invited to be co-chair director of the 2nd World Congress on Advances in COVID with Prof. Malali Gowda from the Bangalore Genomics Center in India. We held this successful event from August 27 to 30, 2020, with the presence of great scientists such as Dr. Andrew Pollard, a friend, director of the Oxford Vaccine, and Dr. Robert Gallo, one of the discoverers of the AIDS virus, among others notable scientists, whom I invited. There I explained in more detail pneumolysis and silent hypoxia (low oxygen), which can lead to sudden death. I spoke not only about microscopic studies but also about the pathophysiology of this terrible disease. Prof. Pelosi presented additional evidence of pneumolysis, confirming its existence. I invited him to participate in 2 conferences with me, here in La Paz. We also published with my daughter Natalia, about pneumolysis in the National Bioethics Bulletin, directed by Dr. Javier Luna Orozco.
The new concept, “Pneumolysis”, developed by me, about the serious commitment caused by the coronavirus in the current COVID-19 pandemic, constitutes a high-risk factor at this time. The coronavirus reaches the lung by inhalation and by entering through the pneumocytes’ ACE-2 receptors (respiratory cells in the lung) nests within. The RNA material of the virus is reproduced and destroys these cells: Pneumolysis (pneumo = lung, lysis = destruction).
The lung pneumolysis in COVID-19
That is why there is a severe injury to various parts of the lung (white areas on the tomography), causing a drop in the oxygen level, evidenced by the digital pulse oximeter. The patients’ lungs are gradually destroyed as the virus spreads, leading to “silent or silent hypoxemia.” Hypoxemia (hypo = low, oxemia = oxygen in the blood) measured with the pulse-oximeter. Returning to the forest burning started by people in the amazon areas. In these circumstances, the smoke in the environment is an incredibly aggravating factor compromising health, particularly those who do not have access to medicinal oxygen, which can cost them their lives. The smoke also blocks the entry of sunlight. Therefore, ultra-violet radiation protects us from the coronavirus, as I stated in the article: The advantages of ultra-violet radiation in controlling the coronavirus in high-altitude (La Razon, April 5, 2020) . Recently by suggestion of the Physicist Roberto Vera we analyzed this in the News Bulletin: ( https://zuniv.net/pub/BOLETIN1Ambiente_13oct.pdf).
Those who manage to survive the attack of the virus, recover. But they may be left with severe pulmonary fibrosis (scarring) that reduces oxygen uptake and reduces their ability to exercise. That is, the lungs are limited in their function. Faced with these circumstances of respiratory failure, the smoke caused by the burns is a seriously aggravating factor that puts the lives of the inhabitants at risk. Furthermore, the lungs of nature are the plants and trees that, through their leaves and by the action of the sun’s rays, generate oxygen on the planet through a cycle of cellular metabolism. By destroying these “lungs of nature” through forest burning, the entire planet’s environment is also seriously compromised. Virtually all animals on the planet need oxygen to survive. That is why, like what has been called Pneumolysis at the pulmonary level (of a micro-environment in our bodies ), we must call Forestalisis (forestal = forest, lysis = destruction), Forestlysis in English, to the destruction of the plants by burning (of the macro-environment). This leads to the compromise of flora and fauna due to direct aggression from burning and the absence of plant-based food sources. PHOTO (OPINION PERIODIC, JULY 19, 2011)
Chaqueo Bolivia
In COVID-19, the coronavirus destroys the human lung ( Pneumolysis ) and causes death. In the burning of the forests, the human being destroys the lung of nature (Forestalysis). The irresponsible people who set fires are the “viruses of the planet ” and those going to destroy it. And in this way, it is a global suicide compromising our lives, all our plants, all our animals, everything, absolutely all ……… life !!!! It is for all this, Bolivian citizens and citizens from all over the world, that we must stop generating uncontrollable fires. Because we are severely hurting mother earth and this Forestalisis (a new terminology that I invent), it can lead our planet to a lethal outcome where everyone and each of us will lose the most valuable jewel in the Universe: Life!
High Altitude Pulmonary and Pathology Institute in La Paz, Bolivia 3500m
As far as we know, we were the first in the world to propose that the U-V at high altitude would be a protective disinfectant in the COVID Pandemic. Originally, in Dec 2017 on a paper on Longevity at high altitude(Se ref. 1, below). Then I wrote a newspaper article about it when the Pandemic started to arrive in Bolivia on April 5th, 2020(3). My daughter Natalia Zubieta-DeUrioste, M.D., and I teamed up with another Bolivian Jorge Soliz Ph.D. and Christian Arias from Laval University who postulated that the lower amount of ACE2 receptors in the lungs at high altitude could also be a protective factor at high altitude. We participated in the U-V section. The other coauthors of that paper were several Bolivian Ph.D. students and an Australian Ph.D. (4). Likewise, we wrote of multiple diseases in COVID-19 early on May 5, 2020 (5) currently under peer review. Furthermore, I created the term “Pneumolysis” to describe what happens in COVID-19 and presented it for the first time in the INTERNATIONAL CONFERENCE ON CORONA VIRAL GENOME, in India (See the banner below). We feel proud to be able to contribute with our knowledge accumulated over 50 years of work at IPPA Just celebrated on July 9th, 2020, to this COVID Pandemic.
20. Winners of the 1st award of the Science and Technology in the area of Medicine and Pharmaceutical Sciences from the Ministry of Health in La Paz, Bolivia based on our publications on lower COVID at high altitude.
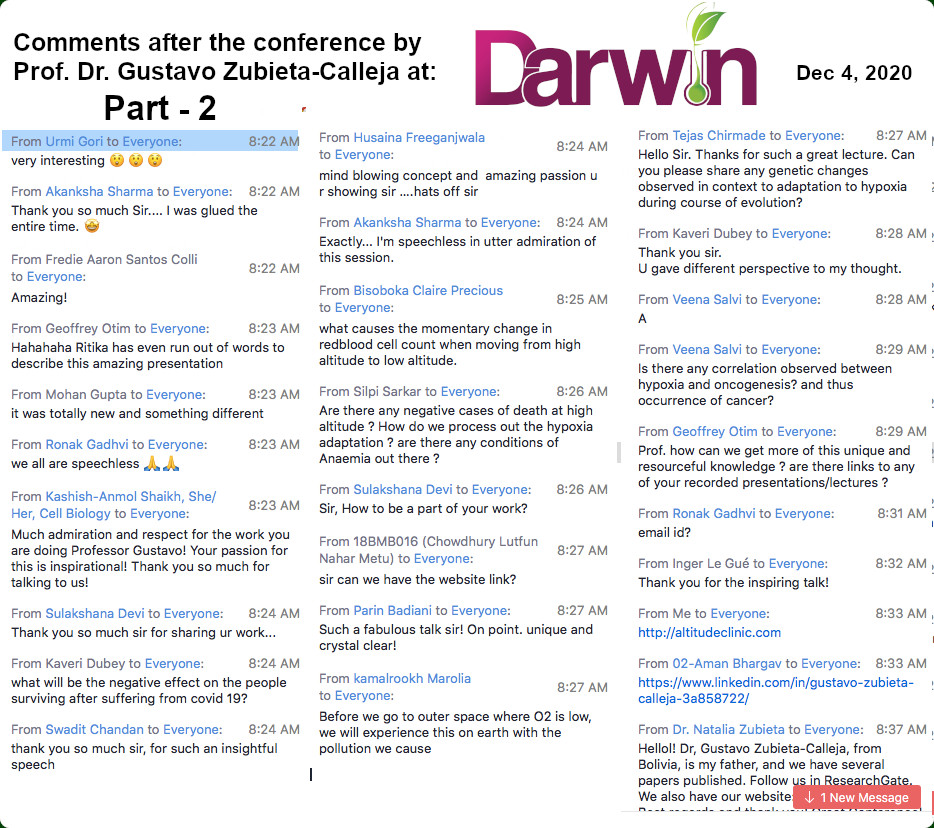
at Darwin 2020, one of India’s Biggest Evolutionary Movements in BiologyFue muy grato compartir con el Dr. Accinelli de distinguida Universidad Cayetano Heredia, en Lima, PerúEn Zoom 500 asistentes y en Facebook mas de 11,000. Click here to join on June 15, 2021
Yesterday on 01.05.2020, at 3.45 pm we had 7th weekly UNESCO COVID-19 Skype meeting.
The title was “The methods of detection of minimal therapeutic doses of drugs for COVID-19 therapy”
Italian Physician Dr. Foletti delivered a presentation on biophysical properties involved in renal functions based on ACE2 which is linked with SARS-COV-2.
There was outstanding input from Prof. Gustavo Zubieta a well-known pulmonologist from La Paz. Prof.Mubaseri, Dr. Sumanta Goswami and Dr. Md. Iqbal Alam contributed significantly on Molecular biology, clinical medicine, and computational biology to understand the deadly virus. 11 physicians and scientists participated in this 2h 30 mins meeting.
Happy to coordinate UNESCO Natural Science COVID-19 video conference under UNESCO Chair Life Science
Prof. Kusal Das BLDE University
Prof. Sinerik Ajrapetyan Dr. Hamid Mobasheri
Dr. Alberto Foletti Prof. Dr. Gustavo Zubieta-Calleja
As everyone on the planet knows, the coronavirus has attacked in a fierce way, due to its high speed of contagion and its physical characteristics. The advanced countries of the first world have suffered the impact in an alarming way. And they are fighting an almost uncontrollable battle.
In Bolivia, the Government has correctly made rapid quarantine decisions, which constitute an essential measure in order to avoid the subsequent overload of medical centers and especially intensive care units, which are very limited.
This is not an easy measure to carry out and understand in its complexity, but it is a fundamental defense mechanism to flatten the incidence curve. That is, instead of being initially exponential or hyperexponential (as I have called it, because it does not double every time, but one person can infect many at once), shooting upwards, it becomes a flattened quasi-logarithmic progression. In other words, a mathematical change occurs, very important in its evolution.
Ultra-violet radiation, a component of light that comes from the sun, is very strong at high altitudes in cities above 3,000 meters above sea level (especially) such as La Paz (3,100-4,100), El Alto (4000-4100), Oruro (3,800) and Potosí (4,000), in Bolivia.
The ultraviolet radiation index (UVindex) is considered to be at extreme levels in La Paz, as we found in a publication with Danish colleagues more than 10 years ago in the following graph, where the top line is La Paz, Bolivia 3,600, and the bottom Copenhagen, Denmark
Radiacion Ultravioleta
Footnote: Kessel, L., Kofoed, PC, Zubieta-Calleja, GR & Larsen, M. Acta Opthalmologica.88 (2): 235-40, March 2009.
As an expert in altitude medicine, I was invited by Prof. Kusal Das to participate in the UNESCO International Forum on COVID-19 with Chairman Prof. Sinerik Ayrapetyan, on Friday, March 27.
Various experts spoke about the molecular characteristics of the coronavirus, of the incidences in their countries, such as Italy, the United States, India and Iran, among others. The mechanisms of action of the virus were analyzed and the search for different treatment techniques was discussed, taking into account many characteristics of the virus.
Next I expose part of what I exposed:
1) Ultraviolet radiation is a protection factor against this virus, because it is lethal. One of the ways the disease is transmitted is because it sits on surfaces where it stays alive for several hours and possibly even days.
But at high-altitude, solar radiation constitutes a sterilizer of all surfaces where the sun falls. That is why the streets in high-altitude cities benefit from this physical characteristic. As an expert, I always said that ultraviolet radiation was beneficial.
Of course, some are afraid of sun exposure because it could lead to skin cancer, but there are no systematic studies to prove these claims. The body adapts to the highest levels of radiation; otherwise people living in the highlands would have a high incidence of cancer, from a long time ago and nowadays.
Quite the contrary, ultraviolet radiation is now a formidable mechanism for our defense against the virus.
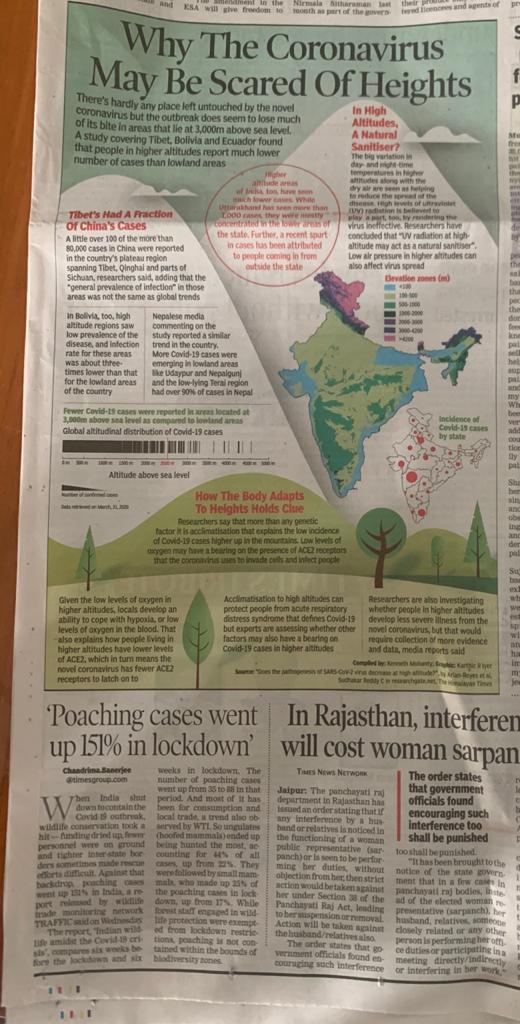
2) Dr. Jorge Solíz, from Laval University, Canada, also observed that in China there were no cases or they were very rare in the Tibet area. Together with other colleagues we are writing a scientific article on this topic. Dr. Kusal Das, from BLDE University, in India, where I am a “visiting professor”, likewise noted that there is lower incidence in high altitude areas in his country.
3) In December 2018 we published with my collaborator Dr. Natalia Zubieta de Urioste an article in relation to the advantages of life at high-altitude, in which we affirm that man lives longer at high-altitude.
We demonstrate this with a longevity graph in all Bolivian cities (based on Segip , local citizen registration office, data), which shows an upward curve starting in Pando at 300m and ending in Potosí at 4100m. In it we also mention the advantages of ultraviolet radiation at high-altitude.
4) Ultraviolet lights are currently being built for use in hospitals and intensive care rooms. Even a Bolivian company in Santa Cruz, whom I congratulate.
5) The low incidence of infections in Oruro, undoubtedly, is due to a strict quarantine (if I’m not mistaken, the first in the country). It deserves our recognition because at the moment the initial eight cases have not increased, with only “patient zero” is an imported case in Oruro).
But I must add that ultraviolet radiation, our ally in high-altitude cities, is also playing an important role. This does not mean, however, that other cases may not appear eventually, because there are many variables, but at the end of this pandemic the statistics will most likely show thatat high-altitude there was a lower incidence.
This does not mean, however, that you must let your guard down. There are also other technical aspects of adaptation to height that we will mention very shortly.
6) On January 30, 2020, in an interview with University Radio-Tv, thanks to a kind invitation from Johnny Villarroel, who directs the Disarmed Discourse program, in which Gonzalo Taboada, president of the Bolivian Academy of Sciences also participated , I stated the following:
That coronavirus treatment centers, with intensive care rooms, should be installed in remote and isolated areas of the cities so as to avoid contamination. I recommended that patients not be taken to centrally located hospitals, leaving them free to care for common illnesses.
In the case of La Paz, I suggested that it be in the highlands, precisely because there is more ultraviolet radiation there. But I also made a recommendation: subsequently, intensive therapy treatment rooms should have a partially glass ceiling, like skylights, to allow ultraviolet light to enter, in order to sterilize the environment in a natural way.
Hopefully in the future the importance of these suggestions will be understood.
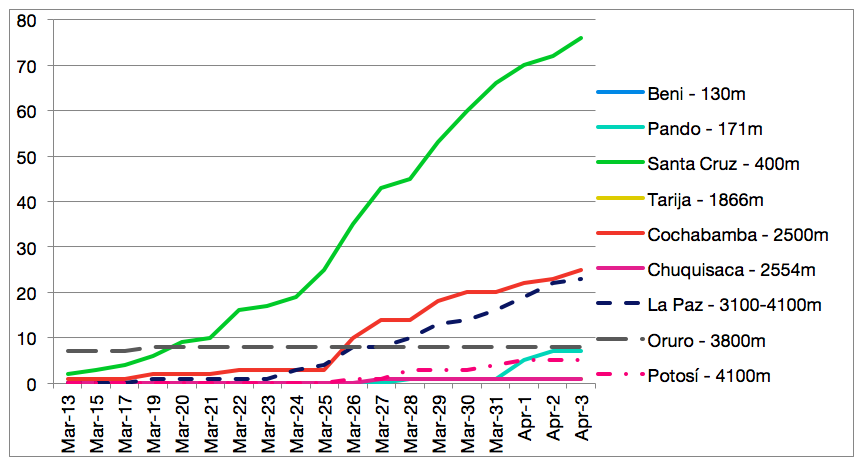
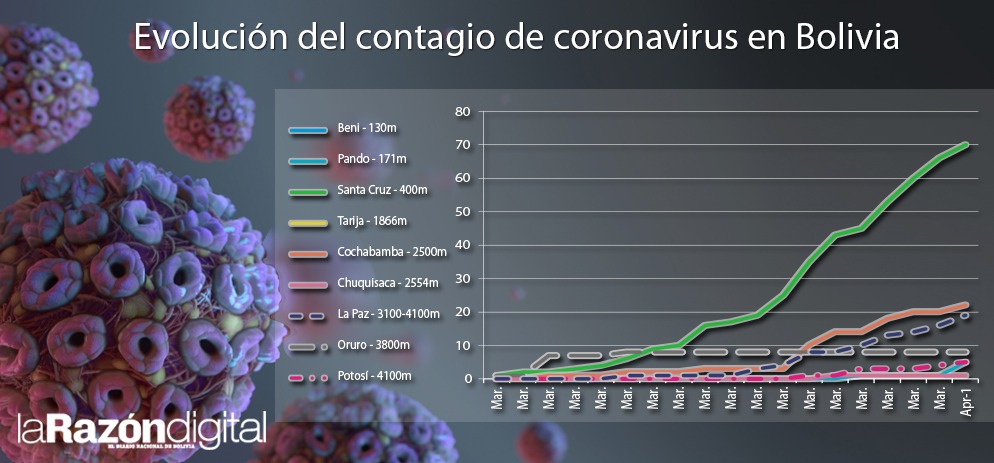
7) The following graph shows the evolution of coronavirus infections in Bolivia in which it is clearly observed that in high-altitude cities (with broken lines) there is less incidence as a function of time:
8) It is also recommended that when someone arrives at home and takes off the clothes used on the street, they should expose them to the sun during this stage. This will allow the virus to be removed quickly (possibly 1/2 hour).
9) It is important to mention that, as inhabitants of the highlands, if one were to suffer a very severe case of CoVid-2 that evolves favorably, thanks to the treatments of the heroic doctors, nurses and health personnel in the highland areas, the consequences of the lung lesions could leave fibrosis (scars), hindering exercise capacity.
These people would develop a Chronic Mountain Sickness (PoliEritroCitemia),in more than a month and a half, which is a compensatory mechanism against chronic respiratory insufficiency, .
Several are likely to be able to stay and develop their lives normally at high-altitude with proper medical care.
Finally, I must add that you should not let your guard down, because although there are fewer cases at altitude, there are cases, of course, and we must all respect the quarantine.
He is a doctor, professor and director of the High Altitude Pulmonary and Pathology Institute (IPPA)
Las ventajas de la radiación ultravioleta en el control del coronavirus en la altura
En Bolivia, el Gobierno ha tomado correctamente decisiones rápidas de cuarentena, que se constituyen una medida esencial a fin de evitar la sobrecarga posterior de los centros médicos y sobretodo de las unidades de terapia intensiva, que son muy limitadas
Como todos en el planeta sabemos, el coronavirus ha atacado de una forma feroz, por su gran velocidad de contagio y sus características físicas. Los países avanzados del primer mundo han sufrido el impacto de una manera alarmante. Y están librando una batalla casi incontrolable.
En Bolivia, el Gobierno ha tomado correctamente decisiones rápidas de cuarentena, que se constituyen una medida esencial a fin de evitar la sobrecarga posterior de los centros médicos y sobretodo de las unidades de terapia intensiva, que son muy limitadas.
Ésta no es una medida fácil de llevar a cabo y entenderla en su complejidad, pero es un mecanismo de defensa fundamental para aplanar la curva de incidencia. Es decir, en vez de que sea inicialmente exponencial o hiperexponencial (como la he denominado, porque no se dobla cada vez, sino una persona puede contagiar a muchos a la vez), disparándose hacia arriba, se la vuelve una progresión cuasi logarítmica aplanada.
Es decir se produce un cambio matemático, muy importante en su evolución. La radiación ultra-violeta, componente de la luz que proviene del sol, es muy fuerte en la altura en las ciudades por encima de los 3.000 msnm (sobretodo) como La Paz (3.100-4.100), El Alto (4000-4100), Oruro (3.800) y Potosí (4000), en Bolivia.
Se considera que el índice de radiación ultravioleta (UVindex) está en niveles extremos en La Paz, como lo constatamos en una publicación con unos colegas daneses hace más de 10 años en la siguiente gráfica, donde la línea delgada es La Paz, Bolivia 3.600, y la gruesa Copenhagen, Dinamarca
Pie de gráfica: Kessel, L., Kofoed, P.C., Zubieta-Calleja, G.R. & Larsen, M. Acta Opthalmologica.88(2):235-40, March 2009.
Como experto en medicina de altura fui invitado a participar en el Forum Internacional sobre COVID-19 de la UNESCO, el viernes 27 de marzo, como único exponente de toda Sudamérica.
Diversos expertos hablaron sobre las características moleculares del coronavirus, de las incidencias en sus países, como Italia, Estados Unidos, India e Irán, entre otros. Se analizaron los mecanismos de acción del virus y se discute la búsqueda de diferentes técnicas de tratamiento, tomando en cuenta muchas características del virus.
A continuación expongo parte de lo que expuse:
1) La radiación ultravioleta es un factor de protección ante este virus, porque le resulta letal. Una de las formas de transmisión de la enfermedad es porque se asienta en superficies donde se mantiene con vida durante varias horas y posiblemente hasta días.
Pero en la altura, la radiación solar se constituye en un esterilizador de toda superficie donde cae el sol. Por eso las calles en las ciudades de altura se benefician de esta característica física de la altura. Como experto, siempre dije que la radiación ultravioleta era beneficiosa.
Por supuesto que algunos tienen miedo de exponerse al sol porque podría producir cáncer de la piel, pero no existen estudios sistemáticos que prueben estas afirmaciones. El organismo se adapta a los niveles más altos de radiación; de otra manera la gente que vive en el altiplano tendría mucha incidencia de cáncer, desde antes y en la actualidad.
Al contrario, la radiación ultravioleta ahora resulta un mecanismo formidable para nuestra defensa ante el virus.
2) El doctor Jorge Solíz, de Universidad de Laval, de Canadá, también observó que en China no hubo casos o fueron muy raros en la zona del Tíbet.
En forma conjunta con otros colegas estamos escribiendo un artículo científico sobre este tema. El doctor Kusal Das, de la BLDE University, en India, donde soy “professor visitante”, también notó que en las zonas de altura en su país hay menor incidencia.
3) En diciembre de 2018 publicamos con mi colaboradora la doctora Natalia Zubieta de Urioste un artículo en relación a las ventajas de la vida en la altura, en el que afirmamos que el hombre vive más largo en la altura.
Lo demostramos con un gráfico de longevidad en todas las ciudades de Bolivia (basada en datos del Segip), que muestra una curva ascendente empezando en Pando y terminado en Potosí.
Allí también mencionamos las ventajas de la radiación ultravioleta en la altura.
4) Actualmente se están construyendo luces ultravioleta para utilizar en los hospitales y salas de terapia intensiva. Incluso una compañía boliviana en Santa Cruz, a la que felicito.
5) La baja incidencia de contagios en Oruro, indudablemente, se debe a una cuarentena estricta (si no me equivoco, la primera en el país), que merece nuestro reconocimiento porque por el momento no han aumentado los ocho casos iniciales, que de los cuales, según tengo entendido, varios fueron importados por viajeros al exterior (ndR: solo la “paciente cero” es caso importado en Oruro).
Pero debo añadir que también está jugando un rol importante la radiación ultravioleta, nuestro aliado en las ciudades de altura. Eso no significa, sin embargo, que no puedan aparecen otros casos eventualmente, porque existen muchas variables, pero al final de esta pandemia las estadísticas muy probablemente demostrarán que en los lugares de altura hubo menor incidencia.
Esto no significa, sin embargo, que se debe bajar la guardia. También existen otros aspectos técnicos de adaptación a la altura que mencionaremos en una futura oportunidad.
6) El 30 de enero de 2020, en una entrevista de Radio-Tv Universitaria, gracias a una gentil invitación de Johnny Villarroel, quien dirige el programa Desarmado Discursivo, en el que también participó Gonzalo Taboada, presidente de la Academia de Ciencias de Bolivia, afirmé lo siguiente:
Que se deben instalar centros de tratamiento del coronavirus, con salas de terapia intensiva, en áreas alejadas y aisladas de las ciudades para no contaminar. Recomendé que no se lleven a los pacientes a los hospitales centralmente localizados, para dejarlos éstos libres para la atención de las enfermedades habituales.
En el caso de La Paz, sugerí que sea en el altiplano, justamente porque allí existe mayor radiación ultravioleta. Pero además hice una recomendación: posteriormente, las salas de tratamiento de terapia intensiva deberían tener el techo parcialmente de vidrio, como unas claraboyas, para permitir el ingreso de la luz ultravioleta, con el fin de producir la esterilización del ambiente en una forma natural.
Ojalá en el futuro se comprenda la importancia de estas sugerencias.
7) La siguiente gráfica muestra la evolución de las infecciones del coronavirus en Bolivia en la que se observa claramente que en las ciudades de altura (con líneas entrecortadas) hay menor incidencia en función del tiempo:
8) También se recomienda que cuando alguien llegue a su casa y se saque la ropa que usó en la calle, debe exponerla al sol durante esta etapa. Esto permitirá que el virus sea eliminado rápidamente.
9) Es importante mencionar que, como habitantes de la altura, si se llegara a sufrir un caso muy severo que al final evolucionara favorablemente, gracias a los tratamientos de los heroicos médicos, enfermeras y personal de salud en las zonas de altura, las secuelas de las lesiones pulmonares podrían dejar fibrosis (cicatrices), dificultando la capacidad para el ejercicio.
Estas personas desarrollarían en el lapso de más de un mes y medio una poliglobulia (PoliEritroCitemia), que es un mecanismo de compensación frente a la insuficiencia respiratoria crónica.
Es probable que varios puedan permanecer y desarrollar su vida normalmente en la altura con un cuidado médico adecuado.
Finalmente, debo añadir que no se debe bajar la guardia, porque aunque son menos los casos en la altura, existen casos y debemos respetar todos la cuarentena.
Otras recomendaciones pueden ser encontradas en línea en nuestra página web: http://altitudeclinic.com/blog
Gustavo Zubieta-Calleja
Es médico, profesor y director del Instituto Pulmonar y Patología en la Altura (IPPA)
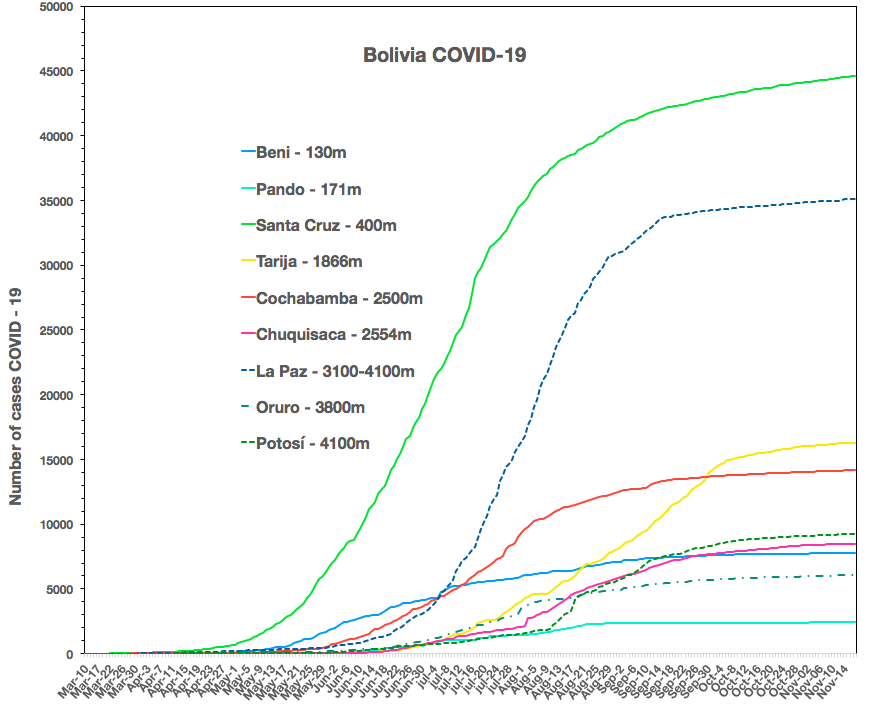
On June 3, 2020, above please note that the incidence in Santa Cruz (2.7 million inhabitants) at 400m above sea level IN GREEN is much higher [12.0 times more] than in the cities of La Paz and El Alto (2.7 million inhabitants) at 3,100m to 4,100mIN DASHED BLUE.
Also, in Beni at 150m IN LIGHT BLUE with only 420,000 inhabitants, (6 times less than in La Paz), already has 3.3 times more cases of COVID-19.
The first graph above is the updated Bolivia SARS-CoVid-2 situation, with the high-altitude low incidence focus. It is linked to our paper
Christian Arias-Reyes1, Natalia Zubieta-DeUrioste2, Liliana Poma-Machicao1, Fernanda Aliaga-Raudan1, Favio Carvajal-Rodriguez1, Mathias Dutschman4, Edith M. Schneider-Gasser3, Gustavo Zubieta-Calleja*2, Jorge Soliz*1,2
1- Institut Universitaire de Cardiologie et de Pneumologie de Québec (IUCPQ), Faculty of Medicine, Université Laval, Québec, QC, Canada. 2- High Altitude Pulmonary and Pathology Institute IPPA. La Paz, Bolivia. 3- Institute of Veterinary Physiology, Vetsuisse-Faculty University of Zurich Winterthurerstrasse 260.
4- Florey Institute of Neuroscience and Mental Health, Gate 11 Royal Parade, 3052, University of Melbourne Victoria, Australia
It is an original idea by Prof. Dr. Gustavo Zubieta-Calleja so that COBID-19 information be up-to-date for all readers of our article until the Pandemia stops. Consequently, this scientific article does not become out-dated. Below, is the incidence difference between the lowland cities in Bolivia and that above 3,000m (dashed lines).
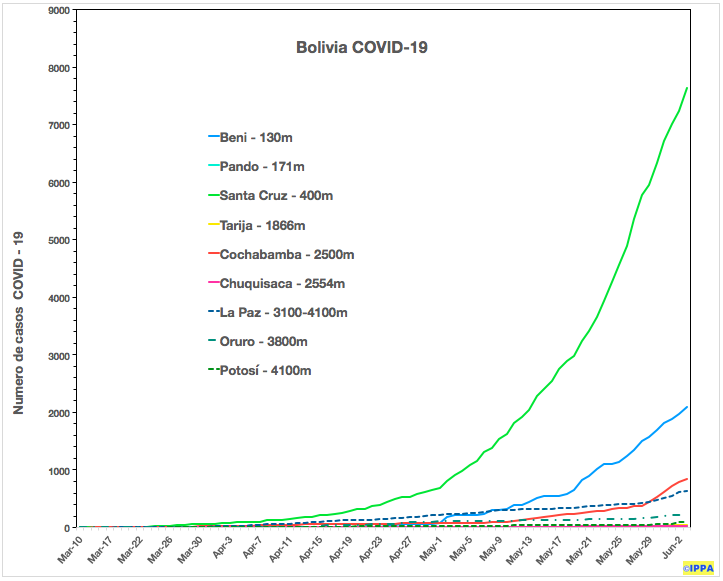
The figure below was developed by Favio Carvajal-Rodríguez.
Bolivia incidence as of April 6th, 2020.
Please read the original newspaper article by Prof. Dr. Gustavo Zubieta-Calleja where he is the first in the world to propose that the Coronovirus will have a lower incidence at high altitude:
Extended Longevity at High Altitude published in Dec 2017 at BLDE J where Prof. Dr. Gustavo Zubieta-Calleja expressed for the first time that at high altitude Ultra-Violet radiation serves as an environmental disinfection. These original concepts gave birth to the concept that Coronavirus can have a lower incidence at high altitude.
In these trying times, ideas on dealing with CoVid-19 in the medical field are mandatory, from any part of the planet. This Pandemia will change, without doubt, the way we scientists deal with population emergency situations in the near future. As a physician working at high altitude, several novel ideas arise, that may aid in the life-saving management of such critical situations. As such, allow me to propose the following:
I suggested that patients with Coronavirus detected at airports or other points of entry should be taken to isolated areas outside cities where vacant buildings ought to be adapted for intensive care (or containers with sunroofs). They should not at all be taken to city or town hospitals as, particularly in a country with limited resources, as they would overwhelm existing intensive care units and thereby displace all work with routine critically ill patients. In addition, it would become a nucleus that spreads the disease to the otherwise healthy population. The areas should be surrounded by open space, with security and the sterilization techniques mentioned in the 3rd point should be applied.
Furthermore, In the city of La Paz, Bolivia (3100-4100m) establishing these modified buildings in the Altiplano (High Plateau) at 4,100 meters above sea level would indeed be beneficial as ultraviolet radiation is relatively high and can help as a natural bio-sterilization resource. Furthermore, the Intensive Care Units (ICUs) should have roofs to let sunlight come through.
The recent good news is that Dr. Augusto Ittig an intensive care specialist in Jujuy, Argentina has established his Coronavirus isolation and intensive care treatment, following theses guidelines.
2) I originally mentioned that there was an exponential growth of this Pandemia. Actually, it is a Hyper-Exponential, since it does not follow the regular exponential progression (y = A * Bx) but rather, in CoVid-19, 1 patient in a closed environment full of people can infect 50 or more in one shot from the very beginning.
3) The management of intensive care units has to be modified. As mentioned in the above interview, the Covid-19 is like a nuclear attack. It could actually be termed a BIO-NUCLEUS ATTACK. Viruses are targeting our nuclear cell areas, in search of self-reproduction, as is well known. Hence, the protection suits for the medical personnel should be full-body impermeable overalls leaving only the face exposed. Goggles, face masks and gloves should, of course, be worn. Upon exiting the Intensive Care Unit, the personnel should pass through a mandatory shower with plenty of soap or other disinfectants, followed by hot drying air for the whole body. This can help reduce significantly the viral transmission. This is similar to radioactive contamination, and it could be termed BIO-ACTIVE CONTAMINATION and we physicians need to evolve urgently to these new 21st-century health safeguarding strategies. After all, we all have the obligation of saving the lives of the courageous intensive care physicians and para-medical personnel that can end up giving their lives in order to save others.
4) Finally, those that actually survive the severe complications with lung (and heart tissue) sequelae will have pulmonary (and perhaps myocardial) fibrosis that will give rise to a pulmonary (and perhaps to some degree, cardiac) insufficiency with resulting complications at a later date. If those patients remain at high altitude, they will present Chronic Mountain Sickness (Poli-erythro-cythemia), as a compensatory mechanism in order to provide sufficient oxygen transport to the tissues. At high altitude, if properly understood, it can be adequately managed.
It has been observed by several groups that Hydroxychloroquine has some effectiveness in the treatment of severe CoVid-19 cases. In-vitro, it has been shown to inhibit the SARS-CoV-2 virus[1,2,3]. The American government has announced that Hydroxychloroquine will be approved by the FDA, ASAP today (March 19, 2020).
We are aware that full studies have to be carried out but, there is no time.
The hospitals are being overflowed, the intensive care units are insufficient, medical resources are running out, even in the first-world countries! People are losing their lives at an alarming rate and the crucial ones turn out to be those of the medical personnel, doctors, nurses, and all those working in the hospitals. The whole planet is shutting down. The world economy is suffering the consequences and above all, it is taking away thousands of human lives.
When you board a plane, prior to departure, you are always told that if there is an emergency related to cabin decompression in-flight, one fundamental advice is:
If you are with a child, please put on the oxygen mask yourself first before putting the child’s mask on. This is a fundamental life-saving procedure since if the loss of consciousness hits the mother or father first then, for certain, not only will the parents lose their lives but also the child.
In a similar manner, if the doctors, nurses and medical personnel fall sick with the Coronavirus, then the patients will also succumb (thousands and maybe tens or hundreds of thousands).
Due to the emergency situation that the whole planet is suffering and particularly the medical and paramedical personnel with this extreme Pandemia, it is essential to consider prevention strategies.
Consequently, we suggest that all medical staff and support teams in hospitals consider start taking Hydroxychloroquine as a preventive strategy, once per week, while studies are being carried out. This is based on the effect of hydroxychloroquine taken to reduce malaria-risk significantly. It is not a perfect solution but it is what is available. The dosage, side-effects, contraindications are available from IAMAT[4]. The long term use of this drug in several other pathologies is well known and apparently well tolerated. We are aware of the criticism that can arise from this. However, today, this world is in a critical emergency situation and the Coronavirus is implacable, unmerciful, selfish and cruel. And we, as physicians from all around the world, have the obligation to help with innovative ideas born from our extensive experience.
The recommended initial dose could be 2 tablets orally for a total of 300mg or 400mg depending on the pharmaceutical presentation STAT, to be repeated every week if no symptoms appear provided there are no contraindications. If SARS-CoV-2 symptoms appear, a full daily dose will probably need to be administered along with the other medication. We cannot wait for full statistically proven studies. Nevertheless, the dosage and methods of administration can be modified with time. What is undeniable is that time is running out !!
The medical personnel should be prioritized. Particularly in a low resource country.
It is highly probable that this emergency life-saving strategy that we propose be considered for immediate execution in all medical personnel treating CoVid-19 hospitals around the world !!!
ESTRATEGIA URGENTE PREVENTIVA CON HIDROXICLOROQUINA PARA EL PERSONAL MEDICO ANTE EL COVID-19.
from: https://www.keckmedicine.org/coronavirus/
Queridos colegas:
Varios grupos han observado que la Hidroxicloroquina tiene cierta efectividad en el tratamiento de casos graves de CoVid-19. In vitro, se ha demostrado que inhibe el virus SARS-CoV-2 [1, 2, 3]. Hoy, 19 de Marzo de 2020, el gobierno estadounidense ha anunciado que la hidroxicloroquina será aprobada por la FDA lo antes posible.
Somos conscientes de que se deben realizar estudios completos, pero no hay tiempo.
Los hospitales se están desbordando, las unidades de cuidados intensivos son insuficientes, los recursos médicos se están agotando, ¡incluso en los países del primer mundo! Las personas están perdiendo la vida a un ritmo alarmante y los que están sufriendo contagios de manera preocupante resultan ser el personal médico, para-médico, enfermeras y todos los que trabajan en los hospitales. Todo el planeta se está paralizando. La economía mundial está sufriendo las consecuencias y sobre todo miles de vidas humanas se están perdiendo.
Cuando Ud. aborda un avión, antes del despegue, siempre le informan que si hay una descompresión de emergencia de la cabina en vuelo, un consejo fundamental es el siguiente:
Si Ud. está con un niño, póngase primero la máscara de oxígeno antes de ponersela al/la niño/a. Este procedimiento es fundamental para salvar vidas, ya que si la pérdida de conciencia golpea primero a la madre o al padre, entonces, con certeza, no solo perderán ellos la vida sino también el/la niño/a.
De manera similar, si los médicos, las enfermeras y el personal médico se enferman con el coronavirus, los pacientes también sucumbirán (miles y quizás decenas o cientos de miles).
Debido a la situación de emergencia que sufre todo el planeta y, en particular, el personal médico y paramédico de esta pandemia extrema, es esencial considerar estrategias de prevención.
En consecuencia, sugerimos que todo el personal médico y los equipos de apoyo en los hospitales consideren comenzar a tomar hidroxicloroquina como estrategia preventiva, una vez por semana, mientras se realizen estudios completos. Esto está basado en la metodología para reducir el riesgo de malaria significativamente. No es una solución perfecta, pero es lo que está disponible. La dosis, los efectos secundarios y las contraindicaciones están disponibles en IAMAT [4]. Tratamientos prolongados para otras patologías con este medicamento, aparentemente son bien tolerados. Somos conscientes de las críticas que pueden surgir de esto. Sin embargo, hoy, este mundo se encuentra en una situación crítica de emergencia y el Coronavirus es implacable, despiadado, egoísta y cruel.
La dosis inicial recomendada podría ser 2 tabletas de 300 mg por vía oral STAT, que se repetirá cada semana si no aparecen los síntomas. siempre que no hayan contraindicaciones. Si aparecieran los síntomas de SARS-CoV-2, probablemente será necesario administrar una dosis diaria completa junto con los otros medicamentos. No podemos esperar a estudios científicos completos estadísticamente comprobados sin embargo, las dosis e indicaciones se podrán mejorar a través del tiempo. Lo irrefutable es que el tiempo se acaba …
Se debe priorizar al personal médico. El tiempo dirá si esta estrategia deba expandirse a toda la población.
¡Es muy probable que esta estrategia de emergencia para salvar vidas que proponemos hoy, sea considerada para su ejecución inmediata en todo el personal médico que trata el Co-Vid-19 en los hospitales de todo el mundo!
Otras ideas fueron expresadasel 30 de Enero de 2020 y luego modificados el 17 de Marzo 2020. Para leerlas haga click aqui.
I arrived with our two daughters, Natalia and Rafaela to Copenhaguen, Denmark on a chilly July back in 2004, in order to join my wife, Lucrecia De Urioste, who was acting as the 1st Secretary in Charge of Consular Affairs at the Bolivian Embassy. Six months previously, when her destiny to go there, had been set, I contacted through the web, Prof. Pouk-Erik Paulev at the Physiology Dept of the Panum Institute of the University of Copenhaguen. He responded “you are welcome in my lab”. From the Embassy, the following day after my arrival, I called Poul-Erik and we spent over an hour talking about our common interests in science. I immediately realized that I had, on the other side of the line, an extraordinary scientist!!
We talked about Ole Siggaard-Andersen, another Dane, the world’s father of acid-base status in blood, whom I admired greatly and with whom Poul-Erik was working. I was truly delighted and amazed! Many years back I had corresponded with Ole, regarding my interest of Acid-base and had even sent him the first computer interpretation of arterial blood gases and acid-base status, that I had written. So I could hardly believe my luck. At the end of our long telephone conversation, Pool-Erik told me to meet him at his office in the Panum Institute, next day.
When I knocked on his door, I found a tall, kind and a very enthusiastic man, with a pleasant smile who welcomed me effusibely. I immediately felt at home. He opened the door next to his Office and said, “this is your Office”. I could hardly believe it
Three and a half years of very productive pleasant scientific collaboration, ensued. We published joint papers related to high altitude, my specialty, in a country where the highest Point is a 170 m. hill.
I learned so much from him, in regards to scientific rigor, synthesis, pragmatism, simple minded attitudes, all, fundamental traits of superior men.
Shown here, a beautiful image of our collaboration at Panum Institute of Physiology, University of Copenhagen
He had been working on a review paper on the extraordinary achievements of the Danish scientists on acid-base equilibrium. I exposed to him the need to make high altitude corrections for the adequate interpretation in all high altitude cities of the world, a knowledge that would save lives. He became immediately interested and when I finished the calculations and the graphs, he decided to include a section in his review article and changed the title to “Essentials in the diagnosis of Acid-Base Disorders and it’s High Altitude Application“. He offered to put my name as first author and I refused. Then, I came up with the idea of tossing a coin, that upon flipping in the air and dropping to the ground, favored him. We laughed and carried on and write in all, 8 papers together.
You can read here an amusing story on the acid-base analyzer at IPPA.
The subjects were diverse including high altitude diving tables. He came to our III Chronic Hypoxia Symposium with his lovely wife Kirsten. Some photos can be seen here.
His generosity went beyond limits. He wrote a physiology book and put it on-line for free use, by anyone. Later on, he granted me co-authorship and I wrote the High Altitude section. Kirsten McCord, one of his patients had discovered his personality and collaborated with him making the graphs, that are now so famous in many physiology books. She went on to become a lifetime collaborator and friend always visiting Poul-Erik and his lovely wife Kirsten that always greeted us with a smile and great Smorebrød (typical Danish sandwiches) at their enchanting home in Birkerød, right next to the golf course, where Poul-Erik and his wife Kirsten, spent many hours enjoying the fields.
I throughly enjoyed discussion of many aspects of physiology and science in his lab. He told me very interesting stories, like when he was a young man and wrote an article that questioned the concepts of Herman Rahn, who was a notable German physiologist who had moved to US. He pointed out that Herman had not been upset, quite the contrary, he invited Poul-Erik to spend some time in his lab. He also told me that Herman had a small scale in his pocket and ran out everyday from his office to the garden to weigh an egg of a small byrd in his nest, that way he was able to study hydration of the egg. That was a time of superior scientists, that made fantastic advances in science. There was no mediocrity, that my father once referred to as: “a congenital disease, very painful and with no treatment”.
Poul-Erik wrote a beautiful and concise biography. I insisted that it be longer, but he was always precise and to the point. It can be read here. Noteworthy is the fact that he suspected decompression sickness when most thought that there was a toxic effect in the water. It is important to note that while at the Panum Institute, I noticed that many of his colleagues were jealous of his work. They had tried to outs him from his teaching on several occasions, but could not do so because he had so many scientific publications, more than any of his colleagues. When I joined him and we worked together, I noticed a lot of jealousy about his work and I of course had to inherit this unnoble attitude towards him. But to simply spend life together with him, and to share the most beautiful moments together, in science and deep nearly parental friendship, was more than welcome.
Poul-Erik had worked as a young scientist, in the study of rescuing sailors from submarines. He performed many dives in a 20 meter pool specially designed in order to develop rescue techniques. He dived so many times that on one occasion upon coming up too fast he developed the “bends” (decompression sickness), that he referred to as very painful. He was immediately put of a hyperbaric chamber where he had to spend many hours and upon exit, he again presented pains so he returned for some more hours. This stimulated his interest in diving physiology. he wrote several papers, and I joined him in a few. We wrote about high altitude diving in Lake Titicaca and higher lagoons. This lead to the creation of the Poul-Erik Paulev High Altitude Laboratory.
There he wrote a most beautiful, concise and admirable autobiography. We travelled jointly to a meeting in Poland to join his friend Pokorsky of the Polish Science Academy. We also went to a meeting in Berlin. He asked me to replace Bengt Saltin in a course on acid-base in the north of Denmark, where we attended jointly with our wives. Thanks to their generosity we were able to integrate our family in the fascinating life of Danish culture, of which we became great admirers. I even wrote an article on Danish education in the Copenhagen Post.
He came with Kirsten, to the III Chronic Hypoxia Symposium that I organized in Bolivia. I created the Poul-Erik High Altitude Diving Laboratory in our building.
There we also met Pernille, Thomas and Matias, wonderful, wonderful Danés, He had 3 daughters and Kirsten has 2 sons.
I have difficulty expressing, when I write these words, about this extraordinary man, of all his scientific and human greatness!!
Had the world been populated by more people like him, we would all live in Paradise.
I express my profound admiration for his extensive and wisdom filled scientific work, of over 160 articles published in prestigious Journals around the world. Many are available at Researchgate.net. What a great Danish Physiologist he was. He left us on July 2017, when he decided it was time time to leave at 84 years of age after aheroic battle with Parkinson’s Disease.
His legacy is scientific, and I bow to always remind all scientists around the world, about his outstanding achievements.
Grand Chronic Hypoxia Tour throughout India July 2016 in the city of Kochi
In this series of consecutive blogs, you can read about this outstanding scientific tour. Each blog is dedicated to one city and one scientific concept presented in the conference “Extraordinary Adaptation to Chronic Hypoxia and Life at High Altitude”.
After visiting Mumbai with its beautiful airport, where we spent the night at a beautiful apartment and a brief tour of the Gateway to India, we flew to Kochi.
The Mumbai Gateway to India
Hosted by Varkey, President of the Lions Club in Kochi, along with his wife, we were given the wonderful surprise that at 10:00 am we could go to the Mariott for a couple of hours to freshen up. It was so beautiful, and so comfortable. Our IPPA team, Prof. Dr. Gustavo Zubieta-Calleja, Lucrecia De Urioste Limariño, Natalia Zubieta De Urioste and Rafaela Zubieta de Urioste, along with our luxury travel team Prof. Thuppil Venkatesh and Prof. Shashisdhara, then moved to the Amrita Hospital, where Gustavo Zubieta-Castillo (Sr) and Gustavo Zubieta-Calleja (Jr) had participated several years back in a conference on Clinical Biochemistry.
Giving the Conference at Amrita Hospital installations
This time again we were warmly greeted at Amrita by Dr. Sanjeev K. Singh, Medical Superintendent.
Natalia giving her interesting comments on chronic hypoxia aspects . Dr. Sanjeev K. Singh 4th from left.
ONE CONCEPT INCLUDED IN THE CONFERENCE “Extraordinary Adaptation to Chronic Hypoxia and Life at High altitude”:
The extraordinary population of a city life La Paz, and El Alto that is like any other matronly in the world. Everyone lives busy and totally unaware of their life at high altitude. They are born here, grow, study, do sports, get married, have children and all in the chronic hypoxia environment uneventfully.
Dr. Thuppil Venkatesh commenting about how high altitude dwellers can suffer from the effects of hyperoxia.
Prof. Dr. Gustavo Zubieta-Calleja’s conference on “Extraordinary Adaptation to Chronic Hypoxia”.
We again visited the unique antique shops in Kochi with the kind hosting of Varkey and his lovely wife Sarada Varkey.
Prof. N. Shashidhara, Lucretia De Urioste and Mrs. Sarada Varkey
Prof. N. Shashidhara, Prof. Thuppil Venkatesh and Prof. Dr. Gustavo Zubieta-Calleja at Kochi.
T.A. Varky, the President of the Lions Club in Kochi and also the director of several Clinical Laboratories. Alongside is Sarada Varkey, his wife.